AstraZeneca’s BAXFENDY Enters the Hypertension Market: Can Aldosterone Synthase Inhibition Outperform Existing Therapies?
Jun 01, 2026
Summary
- In May 2026, the FDA approved AstraZeneca’s BAXFENDY (baxdrostat), the world’s first aldosterone synthase inhibitor (ASI), marking the arrival of an entirely new pharmacological class for a condition that affects 1.4 billion people globally.
- The approval addresses a stubborn clinical gap. Despite existing options like ACE inhibitors, ARBs, and calcium channel blockers, nearly 23 million Americans with hypertension remain uncontrolled even on multiple medications.
- BAXFENDY’s FDA approval is backed by the landmark BaxHTN Phase III trial, which demonstrated a placebo-adjusted reduction of nearly 10 mmHg in systolic blood pressure.
- Baxfendy opens a largely untapped treatment segment and has the potential to redefine standard-of-care protocols for resistant hypertension. The drug is a cornerstone of AstraZeneca’s broader $80 billion revenue target by 2030, underscoring its strategic commercial weight.
- The most direct pipeline threat is lorundrostat by Mineralys Therapeutics, another ASI in development for hypertension, whose New Drug Application (NDA) was accepted by the FDA in March 2026, with a decision expected in December 2026.
It has been more than two decades since a genuinely new class of blood pressure medication reached patients. Hypertension, often referred to as the “silent killer,” affects over 120 million adults in the United States and remains the most significant modifiable cardiovascular risk factor, contributing to more deaths and disability than any other preventable condition. Alarmingly, this burden is projected to rise further, with the number of hypertension patients expected to surpass 130 million by 2036, as per DelveInsight. Despite its widespread impact, the therapeutic landscape has seen limited innovation since the introduction of ACE inhibitors, ARBs, calcium channel blockers, and diuretics
That long drought may finally be over. In May 2026, the FDA approved AstraZeneca’s BAXFENDY (baxdrostat), the world’s first aldosterone synthase inhibitor (ASI) cleared for the treatment of hypertension. It is not merely a new drug; it is the founding member of an entirely new pharmacological class. To understand why BAXFENDY represents such a significant milestone, you first have to understand the scale of the failure that preceded it. Hypertension is extraordinarily common, but controlling it, especially in patients with multiple comorbidities or those already on several medications, is extraordinarily difficult.
Downloads
Click Here To Get the Article in PDF

Recent Articles
- New Clinical Developments in the Pulmonary Arterial Hypertension Treatment Domain
- The Rise of Energy Drinks: Power in a Can or a Health Hazard?
- Idorsia’s Tryvio Success in Hypertension Treatment After J&J ‘Blunder’?
- Ethicon’s ETHIZIA Hemostatic Sealing Patch; FDA Approves Medtronic’s Minimally Invasive Device to...
- World Hypertension day
Sadaf Javed, Functional Head, Forecasting at DelveInsight, said that in the US, approximately 50% of patients already taking multiple antihypertensive medications still struggle with persistently elevated blood pressure, representing a massive, underserved market.
In the United States alone, roughly half of patients with hypertension who are already on multiple antihypertensive drugs still cannot get their blood pressure under control. That translates to roughly 23 million Americans in what clinicians call “uncontrolled” or “treatment-resistant” hypertension territory. These are people who have tried the standard playbook, thiazide diuretics, ACE inhibitors, beta-blockers, calcium channel blockers, and still cannot hit the target.
The consequences are severe. Research has consistently shown that uncontrolled hypertension dramatically elevates the risk of stroke, heart attack, heart failure, kidney disease, and dementia. An observational study tracking nearly 60,000 patients over almost a decade found that a 9.5 mmHg increase in systolic blood pressure correlated with a 30% greater risk of all-cause mortality and a 41% increase in cardiovascular death. Every millimeter matters, and millions aren’t getting enough of them controlled.
The core problem for resistant cases often traces back to a hormonal culprit: aldosterone. This mineralocorticoid hormone, produced in the adrenal glands, regulates sodium and water retention. When aldosterone levels run too high, due to obesity, high salt intake, genetic predispositions, or a condition called primary aldosteronism, blood pressure climbs and stays elevated despite conventional treatment. Existing approaches don’t directly shut down aldosterone production; they merely blunt some of its downstream effects. BAXFENDY attacks the problem at its source.
BAXFENDY’s mechanism is elegantly specific. It is a highly selective, potent oral small molecule that inhibits aldosterone synthase, the enzyme encoded by the CYP11B2 gene, which is directly responsible for synthesizing aldosterone in the adrenal gland. Block this enzyme precisely, and you cut off aldosterone production before it can raise blood pressure.
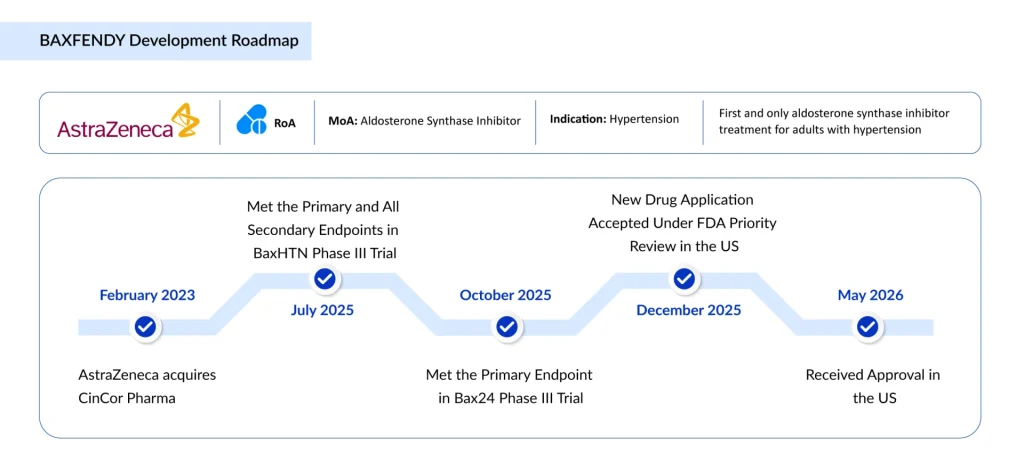
BAXFENDY’s FDA approval rests on data from the BaxHTN Phase III trial, published in the prestigious New England Journal of Medicine in August 2025. The trial enrolled 796 patients in a double-blind, placebo-controlled design and randomized them 1:1:1 to receive BAXFENDY 2mg, BAXFENDY 1mg, or placebo once daily, on top of their existing standard-of-care antihypertensives (at least two agents, including a diuretic). The primary endpoint was the change in mean seated systolic blood pressure (SBP) at week 12.
Why does a nearly 10 mmHg placebo-adjusted reduction matter so much? Because epidemiological data consistently show that a 10 mmHg decrease in systolic blood pressure is associated with approximately a 20% lower risk of major adverse cardiovascular events, strokes, heart attacks, and cardiovascular death. In a condition as prevalent as hypertension, that translates to millions of lives.
The efficacy results were consistent across both the uncontrolled and treatment-resistant subgroups, the very patients who have historically been left behind by existing therapies. Additional confirmatory data came from the separate Bax24 Phase III trial, published in The Lancet in March 2026, which demonstrated a statistically significant and clinically meaningful reduction in 24-hour ambulatory systolic blood pressure in patients with resistant hypertension.
Persistence of efficacy was confirmed through a randomized withdrawal period (weeks 24–32), where patients re-randomized to placebo after responding to BAXFENDY saw their blood pressure rise again, validating that the drug’s effects were real and maintained over time.
BAXFENDY is approved as an add-on therapy; it is indicated in combination with other antihypertensive drugs for adults with hypertension who are not adequately controlled on existing agents. It is not a first-line, standalone treatment. The recommended standard dose is 2 mg orally once daily. For patients at increased risk of hyperkalemia or hyponatremia, the recommended starting dose is 1 mg once daily. The drug was originally discovered and developed by CinCor Pharma, which AstraZeneca acquired in February 2023 for $1.3 billion, a bet that has now paid off handsomely with a landmark first-in-class FDA approval.
| BAXFENDY vs. Existing Therapies | |||
| Drug Class | Mechanism | Typical SBP Reduction | Key Limitation |
| ACE Inhibitors/ARBs | Block renin-angiotensin system | ~8–12 mmHg | Does not block aldosterone production (aldosterone escape) |
| Calcium Channel Blockers | Reduce vascular smooth muscle contraction | ~8–10 mmHg | Does not address aldosterone-mediated resistance |
| Thiazide Diuretics | Promote sodium/water excretion | ~6–10 mmHg | Metabolic side effects; not root-cause treatment |
| MR Antagonists (e.g., spironolactone) | Block the aldosterone receptor | ~7–10 mmHg | Non-selective; gynecomastia, hyperkalemia risks |
| BAXFENDY (Baxdrostat) — NEW | Inhibits aldosterone synthase (CYP11B2) | ~14–16 mmHg (absolute); ~9–10 mmHg placebo-adjusted | Requires potassium/sodium monitoring; add-on only |
The comparison tells a compelling story. Where existing agents compensate for or partially blunt aldosterone’s effects, BAXFENDY cuts off its production at the enzymatic source. This upstream approach matters most in patients whose hypertension is aldosterone-driven, precisely the treatment-resistant population that has run out of options under the current standard of care.
Crucially, BAXFENDY is designed to work alongside existing drugs, not replace them. This positions it not as a competitor to ACE inhibitors or ARBs, but as a complementary agent that addresses an overlooked hormonal pathway when first-, second-, and third-line options have been exhausted.
What makes BAXFENDY particularly interesting from a long-term commercial and clinical standpoint is its potential reach beyond a single indication. AstraZeneca is actively developing the drug across a constellation of cardiorenal conditions where aldosterone dysregulation plays a role:
Primary Aldosteronism (BaxPA trial): A condition caused by overproduction of aldosterone from the adrenal glands, often leading to severe, refractory hypertension and organ damage. BAXFENDY, as a monotherapy here, could be transformative, directly tackling the disease’s hormonal root cause.
Chronic Kidney Disease (CKD) + Hypertension: Two separate Phase III trials are evaluating BAXFENDY in combination with dapagliflozin (AstraZeneca’s own blockbuster SGLT2 inhibitor) in patients with CKD and elevated blood pressure, a synergistic combination targeting both metabolic and hormonal drivers of kidney progression.
Heart Failure Prevention (Prevent-HF): A Phase III study is examining whether BAXFENDY plus dapagliflozin can prevent the development of heart failure in patients with hypertension, one of the most ambitious and potentially high-value indications in cardiovascular medicine.
AstraZeneca is not alone in recognizing the opportunity. Close on its heels is Mineralys Therapeutics, which is developing its own aldosterone synthase inhibitor, lorundrostat, also for hypertension. The FDA accepted Mineralys’s New Drug Application for lorundrostat in March 2026, with a decision expected in December, meaning BAXFENDY could face a credible class competitor within months of its launch.
The first-mover advantage in a newly opened drug class is historically meaningful: it shapes prescriber habits, payer formulary placement, and real-world evidence generation. AstraZeneca has a significant head start, not just in regulatory timing, but in the breadth of its clinical program and the established muscle of its cardiovascular commercial infrastructure. How Mineralys differentiates lorundrostat in terms of safety, dosing convenience, or specific sub-populations will be the defining commercial question of the coming years.

Downloads
Article in PDF
Recent Articles
- One of the leading causes of blindness, and a sight-threatening disease, Uveitis, now has novel t...
- The Rise of Energy Drinks: Power in a Can or a Health Hazard?
- World Hypertension day
- Nascent Advancements and Emerging Therapies in Chronic Pulmonary Hypertension Treatment Market
- Immunocore’s Kimmtrak; Samsung Acquires Biogen’s Biosimilar Unit; Novavax’s COVID-19 Vaccin...



