The Future of Degenerative Disc Disease Treatment: Moving Beyond Symptom Relief with Cell Therapy
Jul 03, 2026
Table of Contents
Summary
- In the US, chronic low back pain affects about 28% of the population, and DDD is estimated to account for roughly half of specific CLBP cases, or around 14 million diagnosed prevalent cases in 2025.
- Standard care includes pain relief, NSAIDs, physical therapy, lifestyle changes, injections, and surgery, but these approaches rarely restore disc structure or prevent further degeneration.
- Cell-based regenerative therapies are gaining attention because they may reduce inflammation, support extracellular matrix repair, and activate endogenous healing within the disc microenvironment.
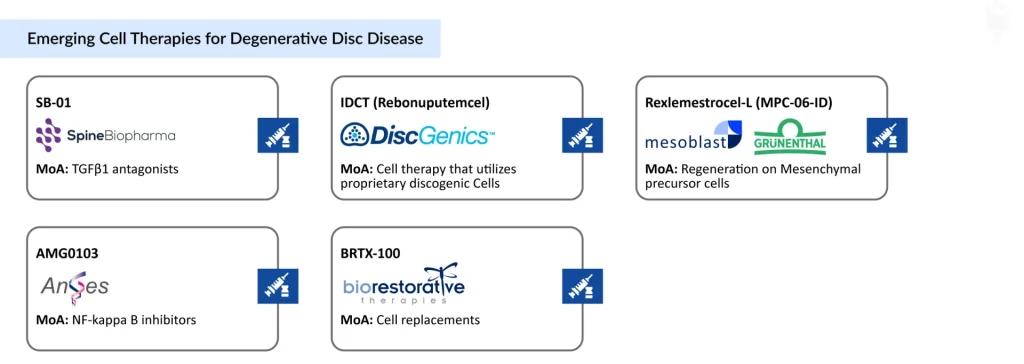
- Several programs are advancing in lumbar DDD, including IDCT (DiscGenics), Rexlemestrocel-L (Mesoblast and Grünenthal), BRTX-100 (BioRestorative Therapies), and other emerging candidates, reflecting strong interest in biological spine repair.
Degenerative Disc Disease (DDD) is one of the leading causes of chronic low back pain and disability worldwide, imposing a substantial clinical, economic, and societal burden. Despite its prevalence, current treatment approaches largely focus on symptom management rather than repairing damaged discs or slowing the underlying degenerative process. Consequently, many patients continue to experience persistent pain, functional limitations, and progressive disease despite receiving standard care.
Downloads
Click Here To Get the Article in PDF

Recent Articles
- Zepp Health Launched OTC Hearing Aids; Neoss Launched NeoScan 2000; FDA Clearance for AI-Assisted...
- Emerging Therapies in the Chronic Pain Pipeline Transforming the Chronic Pain Market Landscape
- Chronic Lower Back Pain: Navigating the Complexity of a Global Epidemic
- Chronic Lower Back Pain Therapy Market
- Chronic Lower Back Pain Market Analysis
According to DelveInsight’s epidemiological estimates, chronic low back pain (CLBP) affects approximately 28% of the US population, with nearly 38% of cases classified as specific CLBP. DDD accounts for roughly half of these specific CLBP cases, representing an estimated 14 million diagnosed prevalent cases in the US in 2025. Disease severity analyses indicate that mild DDD constitutes approximately 70% of cases, followed by moderate (23%) and severe disease (8%), suggesting that most patients are diagnosed before progression to advanced degeneration.
The epidemiological profile of DDD reveals significant variation across sex, age groups, and anatomical regions of the spine. Women bear a greater disease burden than men, accounting for approximately 56% of cases compared with 44% among males. The prevalence of DDD increases markedly with age, with nearly 69% of cases occurring in individuals aged 60 years and older, highlighting the strong association between disc degeneration and aging. Anatomically, lumbar DDD represents the most common subtype, comprising approximately 67% of all cases, followed by cervical (21%) and thoracic DDD (12%). The predominance of lumbar involvement is largely attributed to the substantial mechanical loading and biomechanical stresses experienced by the lower spine, establishing lumbar DDD as the major driver of disease burden, healthcare resource utilization, and associated disability in the United States.
The Limitations of Today’s Degenerative Disc Disease Treatment Paradigm
Management of DDD typically follows a stepwise treatment approach that includes conservative, regenerative, and surgical interventions depending on symptom severity and disease progression. Initial management generally consists of analgesics, Nonsteroidal Anti-inflammatory Drugs (NSAIDs), physical therapy, exercise programs, weight management, and complementary therapies such as acupuncture.
Although these interventions can provide meaningful symptom relief, they do little to alter the biological processes responsible for disc degeneration. For patients with persistent symptoms, epidural injections or surgical procedures may become necessary. However, even these interventions often fail to restore native disc structure or prevent continued degeneration.
This therapeutic gap has created a substantial unmet need for disease-modifying DDD treatments capable of preserving disc integrity while providing durable clinical benefit.
Why are Cell Therapies Attracting Attention?
Regenerative medicine has emerged as one of the most promising areas of innovation in DDD. Among regenerative approaches, cell-based therapies are generating particular interest because they directly target the biological mechanisms driving degeneration. Degenerated intervertebral discs exhibit reduced nucleus pulposus cell density, impaired extracellular matrix production, and elevated levels of inflammatory mediators such as TNF-α and IL-1β. Increased activity of matrix-degrading enzymes further accelerates tissue breakdown and structural collapse.
Cell therapies are designed to interrupt this cycle through multiple mechanisms. Transplanted cells may suppress inflammation, stimulate extracellular matrix synthesis, inhibit catabolic signaling pathways, and activate endogenous repair mechanisms. Increasingly, evidence suggests that these benefits may arise through powerful paracrine signaling effects that reshape the local microenvironment and promote tissue regeneration.
Unlike conventional therapies that primarily address symptoms, cell therapies offer the potential to modify disease progression and restore disc function.
Lumbar DDD: The Primary Target for Regenerative Innovation
The current development pipeline underscores the clinical importance of lumbar DDD. Most investigational regenerative therapies are being developed specifically for patients with lumbar disc degeneration with chronic low back pain.
Programs such as Rebonuputemcel (IDCT) and BRTX-100 are focused on lumbar disease because of its high prevalence and substantial unmet medical need. This concentration of pipeline activity highlights lumbar DDD as the most clinically impactful and commercially significant segment within the broader DDD market.
Rebonuputemcel (IDCT) – DiscGenics: Building the Case for Disc Regeneration
Among the most advanced regenerative programs, IDCT has emerged as one of the strongest demonstrations of biological repair in patients with symptomatic mild-to-moderate lumbar DDD.
The allogeneic injectable cell therapy is designed to address inflammation, promote tissue regeneration, and restore disc function. Clinical studies have reported statistically significant and clinically meaningful improvements in pain, physical function, and quality of life. Patients receiving high-dose treatment achieved greater than 60% reductions in back pain scores, with benefits maintained through 2 years of follow-up. Importantly, improvements exceeded established Minimal Clinically Important Difference (MCID) thresholds across multiple endpoints.
Perhaps most notable is the observation of statistically significant increases in disc volume at one and two years following treatment. These findings provide evidence that IDCT may support true structural regeneration rather than merely symptom control. The therapy has received both Fast Track and Regenerative Medicine Advanced Therapy (RMAT) designations from the US FDA, positioning it among the leading late-stage regenerative assets in DDD.
Rexlemestrocel-L-Mesoblast: Demonstrating Long-term Durability
Mesoblast’s Rexlemestrocel-L represents one of the most extensively studied mesenchymal stem cell approaches in DDD. Derived from allogeneic mesenchymal precursor cells, the therapy has demonstrated durable pain reduction lasting up to three years following a single intradiscal injection. Clinical outcomes suggest that earlier intervention may yield greater benefits, particularly before irreversible structural damage occurs.
A notable finding from long-term studies was the reduction in opioid dependence, with more than one-quarter of opioid users discontinuing treatment by 36 months. Such results highlight the potential for regenerative therapies to reduce reliance on chronic pain medications while delivering sustained clinical improvement.
Emerging Competitors Expanding the Pipeline
Several additional degenerative disc disease programs are contributing to the rapidly evolving regenerative landscape. BRTX-100 employs an autologous cell therapy approach, potentially minimizing immune compatibility concerns while offering a personalized treatment strategy. CELZ-201-DDT has generated encouraging early-stage results and could emerge as a competitive platform if larger studies validate its clinical outcomes.
Meanwhile, next-generation candidates such as TG-C and CybroCell are exploring novel regenerative mechanisms aimed at improving cell survival, enhancing extracellular matrix restoration, and maximizing tissue repair within the challenging disc microenvironment.
Comparing the Leading Cell Therapy Candidates
Although cross-trial comparisons should be interpreted cautiously, distinct strengths are emerging among leading programs. IDCT currently offers some of the strongest evidence for structural regeneration, supported by measurable increases in disc volume and durable clinical improvement. Rexlemestrocel-L provides perhaps the most mature evidence of long-term durability, with benefits extending for at least three years and meaningful reductions in opioid use. BRTX-100’s autologous approach offers personalization advantages, while CELZ-201-DDT remains an intriguing early-stage competitor with encouraging efficacy signals.
From a commercialization standpoint, allogeneic therapies such as IDCT, Rexlemestrocel-L, and CELZ-201-DDT may offer advantages over patient-specific autologous approaches due to their greater scalability, more consistent manufacturing processes, and wider potential accessibility. Among these therapies, IDCT and Rexlemestrocel-L are anticipated to launch in 2028, while BRTX-100 is expected to enter the market in 2029.
Looking Ahead: The Shift toward Biological Spine Repair
The treatment paradigm for DDD may be approaching a pivotal transition. For decades, management strategies have focused largely on symptom control through medications, rehabilitation, injections, and surgery. Emerging cell therapies are challenging this paradigm by targeting the underlying biology of degeneration.
Future success will depend on identifying the patients most likely to benefit, refining degenerative disc disease treatment protocols, and integrating advanced imaging and biomarkers into clinical decision-making. Combination approaches involving biomaterials, growth factors, gene therapies, and tissue-engineered scaffolds may further enhance regenerative outcomes.
Although questions remain regarding durability, reimbursement, and patient selection, the growing body of clinical and imaging evidence suggests that regenerative medicine is moving DDD beyond symptom management. If ongoing late-stage studies continue to deliver positive results, cell therapies could become the first truly disease-modifying interventions capable of preserving spinal function and altering the natural course of DDD.

Downloads
Article in PDF
Recent Articles
- Chronic Lower Back Pain Market Analysis
- Chronic Lower Back Pain: Navigating the Complexity of a Global Epidemic
- Chronic Lower Back Pain Therapy Market
- Zepp Health Launched OTC Hearing Aids; Neoss Launched NeoScan 2000; FDA Clearance for AI-Assisted...
- Emerging Therapies in the Chronic Pain Pipeline Transforming the Chronic Pain Market Landscape



