Tackling Nausea and Vomiting Induced by Motion Sickness
Oct 06, 2023
Table of Contents
There has been an unprecedented explosion in travel in recent years as a result of greater affordability and opportunities. Comfort has become an important element of travel with products such as pillows, eyeshades, and noise-cancelling headphones promising better sleep and reduced stress. Despite these, some people may experience dizziness, nausea, vomiting, etc. – also known as motion sickness.
Moreover, advancements in science such as virtual reality and augmented reality (AR) provide thrilling new experiences that seem to remove the users from their physical reality but also cause some amount of disorientation and physical discomfort that manifest into motion sickness symptoms.
Downloads
Click Here To Get the Article in PDF

What is motion sickness and what are its symptoms?
Motion sickness is a common physiological response that occurs when there is a sensory mismatch between the visual and vestibular systems. It is also known as kinetosis or travel sickness and usually manifests during air, car, bus, train, or boat travel. Despite travel, motion in giant wheels, virtual reality experiences, and other simulators can trigger motion sickness in individuals not used to the disorienting effects. All these can lead to a diverse range of symptoms from nausea and vomiting to cold sweating, pale skin, dizziness, irritability, pallor, headache, drowsiness, yawning, loss of appetite, and increased salivation.
Nausea and vomiting are the hallmarks and the most common symptoms of motion sickness, nausea is a sensation or discomfort in the stomach that signals imminent emesis, while vomiting is the forceful removal of gastrointestinal contents. The sensation of nausea and the ability to vomit are key components of human defenses against uncomfortable conditions like motion sickness or unintentional ingestion of noxious material. Usually, individuals with motion sickness present mild to moderate self-limited symptoms; once the triggering motion ceases, symptoms often resolve entirely within 24 hours.
Besides motion sickness, problems like stomach complications, medications, pregnancy, and pre-existing medical conditions (migraines, inner ear disorders, acute gastritis, anxiety, depression, etc.) can also cause nausea and vomiting.

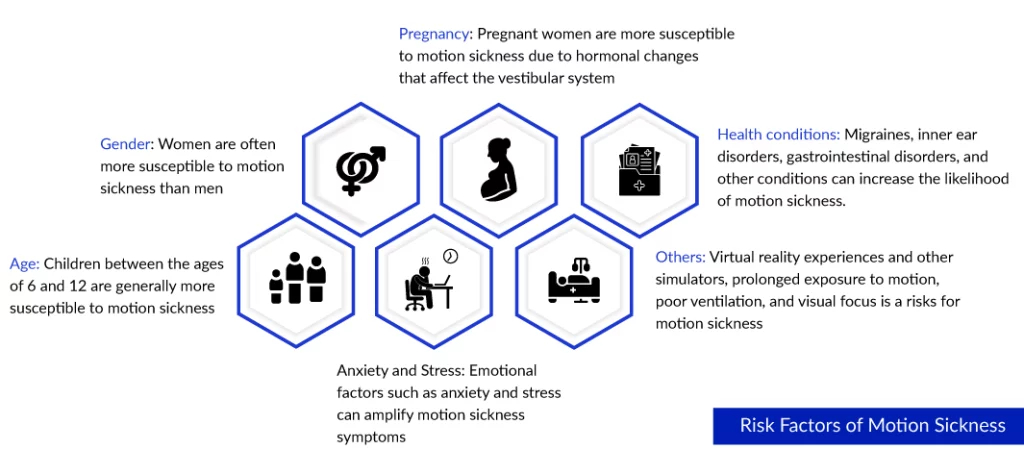
Potential risk factors of motion sickness
Some individuals are more prone to motion sickness than others. Children between the ages of 2 and 12, pregnant and menstruating women, and people with preexisting medical conditions are more susceptible. Further, concurrent medications and taking hormone replacement therapy or oral contraceptives have also been identified as potential risk factors. On the contrary, patients with a total loss of labyrinthine function are immune to motion sickness, and over time, multiple exposures to motion sickness triggers result in habituation, and the individuals can become symptom-free. Dehydration, electrolyte imbalance, anxiety, and depression are some common complications that may occur.
Epidemiology scenario of motion sickness
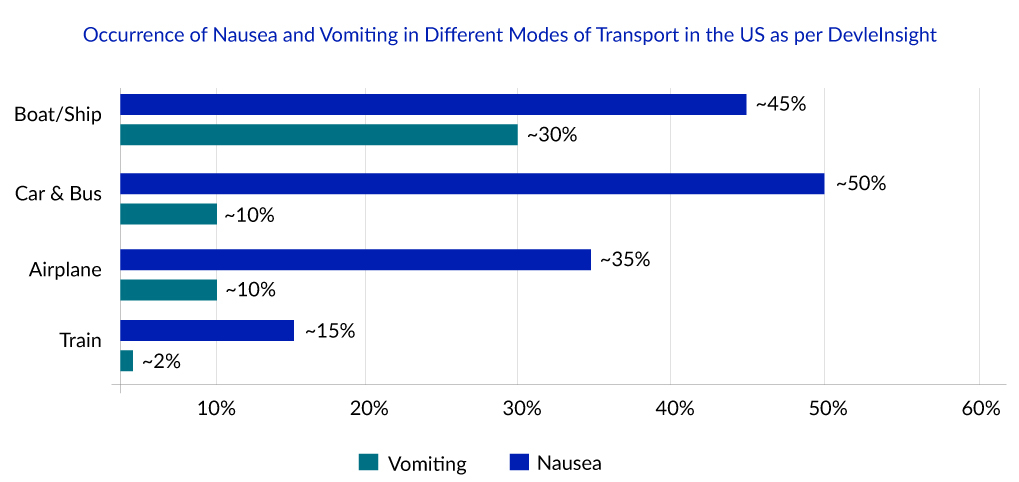
While it is not a serious medical condition, it affects people of all ages and can impact travel plans and activities. Almost every person with fully functional physiological systems develops motion sickness at some point in their lives; however, its occurrence varies significantly depending on the mode of transport, individuals’ susceptibility, and factors such as age and gender. Literature review suggests that cars and buses are the most commonly used transport and have the highest occurrence rate of motion sickness, while the least used transport, boats or ships has the lowest occurrence. According to DelveInsight’s latest published report titled “Nausea And Vomiting Induced By Motion Sickness Epidemiology Forecast”, more than 100 million individuals in the US were affected by motion sickness in 2022.
Common remedies to manage nausea and vomiting in motion sickness
After diagnoses through symptomatic evaluation, medical therapy, self-care, or preventive measures are adopted. Even though motion sickness is a highly prevalent condition, no highly effective medication has yet been developed. Treatment involves a combination of preventive measures, lifestyle changes, and medications. The market for nausea and vomiting induced by motion sickness is largely dominated by over-the-counter (OTC) medications and generic forms of medications, including antihistamines, anticholinergics, benzodiazepines, dopamine receptor antagonists, and others. The only approved drug is TRANSDERM SCOP (scopolamine), a transdermal system patch approved in 1997; since then, the US FDA has not approved any other treatment for the sickness.
TRANSDERM SCOP is an effective agent that prevents nausea and vomiting by inhibiting input to the vestibular nuclei. It is applied in the postauricular area or back of the ear for 4 hours before an antiemetic effect is required and can be used for up to 3 days. For more prolonged use than 3 days, removing the current patch and placing a new one behind the other ear is recommended. However, the therapy is limited by side effects like dry eyes/mouth, photosensitivity, blurred vision, dizziness, headache, and sedation. It is not recommended for children under 12 and is used cautiously in older adults. Some other common medications used in nausea and vomiting induced by motion sickness management include dimenhydrinate, chlorpheniramine, meclizine, prochlorperazine, metoclopramide, ondansetron, and domperidone. However, the efficacy of these medicines is limited, and unwanted side effects may appear.
According to DelveInsight’s estimates, the total nausea and vomiting induced by motion sickness market size in the seven major markets (the United States, Germany, France, Italy, Spain, the United Kingdom, and Japan) is expected to reach a mark of USD 2,000 million by 2032 owing to increasing prevalence and optimistic launches of emerging therapies.
Besides medical treatment, other preventive and management strategies include herbs and supplements, behavioral and postural modification, and acupressure techniques. However, no credible studies show that these techniques work. Herbs like ginger, peppermint, black horehound, and homeopathic remedies like Borax, Cocclus, Nux Vomica, and Petroleum are used. Modifying sensory patterns responsible for the neural mismatch signal by adopting short-term maneuvers like minimum head movement, restricting head movements during vehicle acceleration, focusing on a stable horizon, and mindful breathing helps prevent motion sickness.
Gaps and unmet needs of nausea and vomiting in motion sickness
- Deeper knowledge of the pathophysiology of motion sickness is needed. A lot is known about the neuroanatomy and neurochemistry of vomiting. Although the current knowledge of the cerebral circuits causing nausea exists, it is still quite elementary. Despite being closely associated, central pathways of nausea and vomiting appear to be partly different.
- The lack of epidemiology data makes it difficult to estimate motion sickness occurrence and acts as a hurdle in garnering sufficient consideration. Hence, there is a need to conduct more research and studies to understand the pathophysiology and epidemiology of motion sickness to develop novel preventive and treatment therapies.
- There is a need to refine animal models that better mimic human experiences of nausea and vomiting to understand its pathophysiology and support clinical trials. Even though rats are non-emetic animals, they have been used extensively to explore the neurochemistry of nausea using various behavioral methods. Further advances in neuroscience, genetics, and the integration of various models (cellular, animal, and human) can help bridge the gap between animal findings and clinical applications.
- Discovering a potential biomarker that can objectively detect and emit similar responses to humans in animal models, is needed to pave the way for developing effective anti-nausea medication.
Emerging therapies to provide relief from nausea and vomiting induced by motion sickness
Research and development for drugs for nausea and vomiting in motion sickness is restricted, and the current emerging pipeline remains limited, with only a few trials. Defender Pharmaceuticals and Vanda Pharmaceuticals with Eli Lilly are working to bring novel therapies that can fulfill the unmet need of motion sickness.
Defender Pharmaceuticals, in collaboration with the US Navy and NASA, has developed DPI-386, a nasal gel formulation of scopolamine that allows rapid vascular uptake and potentially direct absorption into the central nervous system and potentially overcome the shortcomings of the oral and patch delivery of scopolamine. The company has submitted the New Drug Application; however, the decision is pending from the US FDA on the acceptance of the application and approval of the drug.
The second drug, i.e., VLY-686 (tradipitant), under investigation by Vanda Pharmaceuticals, is a neurokinin-1 (NK-1) receptor antagonist with the potential to improve the symptoms of motion sickness. Although tradipitant was superior to placebo in preventing vomiting in a Phase III trial, additional positive safety and efficacy data from ongoing Phase III is needed to pave the way for approval.
If approved, these two drugs could be of immediate value to common travelers, professionals, and military personnel in treating and preventing vomiting in motion sickness.

Downloads
Article in PDF



