Warm Autoimmune Hemolytic Anemia Epidemiology forecast segmentation, treatment approaches, and WAIHA market forecast
Apr 03, 2020
As per DelveInsight’s Warm Autoimmune Hemolytic anemia Epidemiology forecast and analysis, WAIHA prevalence in the 7MM was estimated to be around 82,045 cases.
Autoimmune hemolytic anemia (AIHA) – a rare acquired autoimmune disease – is a consequence of dysfunction in the immune system, as a consequence of which the immune system attacks its red blood cells considering them foreign substances. The rate of auto-antibodies finishing off autologous red blood cells is so rapid that the bone marrow fails to cope up, resulting in accelerated destruction of RBCs. The antibodies are primarily IgG that reacts with the proteins on the surface of RBCs giving a positive Coombs test at an optimal temperature.
Primary symptoms of the disease are more or less similar to that of anemia, including fatigue, difficulty breathing, jaundice, and dark urine. In severe disease, fever, chest pain, syncope or heart failure may occur. Hemolysis (the breakdown of red blood cells) occurs mainly in the spleen, so mild splenomegaly is relatively common.
Downloads
Click Here To Get the Article in PDF
As per Orphanet, the annual Autoimmune hemolytic anemia incidence is estimated be around 1/35,000-1/80,000 in North America and Western Europe.
Autoimmune hemolytic anemia (AIHA) is a relatively uncommon disorder with an estimated incidence of 0.8–3 per 105/year in adults, a prevalence of 17:100,000 and a mortality rate of 11%, estimated another study by Petz LD et al.
However, Warm autoimmune hemolytic anemia is the most common form of autoimmune hemolytic anemia.
Warm Autoimmune hemolytic Anemia Epidemiology Analysis
On the basis of Temperature, these auto-antibodies bind with RBCs, Autoimmune hemolytic anemia is classified into Cold Autoimmune hemolytic anemia and Warm Autoimmune hemolytic anemia.
In Warm AIHA, hemolysis takes place at 37 °C (98.6 °F), whereas, in case of Cold AIHA, the reaction takes place at a temperature lower than body temperature.
Out of total AIHA cases, warm Autoimmune hemolytic anemia for 60-70% of the total AIHA cases, cold Autoimmune hemolytic anemia account for 13-15% of the total Autoimmune hemolytic anemia cases. In addition to this, mixed Autoimmune hemolytic anemia cases occur in less than 10% of the cases.
As per a study by Petz LD et al., annual Warm Autoimmune hemolytic anemia Incidence is estimated to be around one per 75,000-80,000 population, occurring in people of all ages.
On the basis of the rate of hemolysis and the severity, Warm Autoimmune hemolytic anemia is categorized as mild to severe and life-threatening.
On the basis of manifestation and complication behind the disease, Warm autoimmune hemolytic anemia is sub-classified into Primary, Secondary and Idiopathic. If the disease is not because of some other illness, it is termed as primary WAIHA. In case, the reason is manifestation or complication of another disease, it is referred to as secondary WAIHA, and in cases, where the cause remains unclear, it is known as idiopathic WAIHA.
Per a study by Valent P et. Al 2008, 50% of the total Warm autoimmune hemolytic anemia cases can be idiopathic, 20% of WAIHA case can be secondary due to lymphoproliferative syndromes, and other 20% can be because of autoimmune diseases. Infections and tumor can also be the reasons for Warm autoimmune hemolytic anemia.
As per the NORD, Warm Autoimmune hemolytic Anemia can afflict people of any age. However; it is more prevalent in adults with a peak incidence between 50-70 year.
Warm Autoimmune hemolytic Anemia Forecast and Analysis
As per the analysis by DelveInsight, Warm Autoimmune hemolytic Anemia prevalence in the 7MM was estimated to be around 82,045.
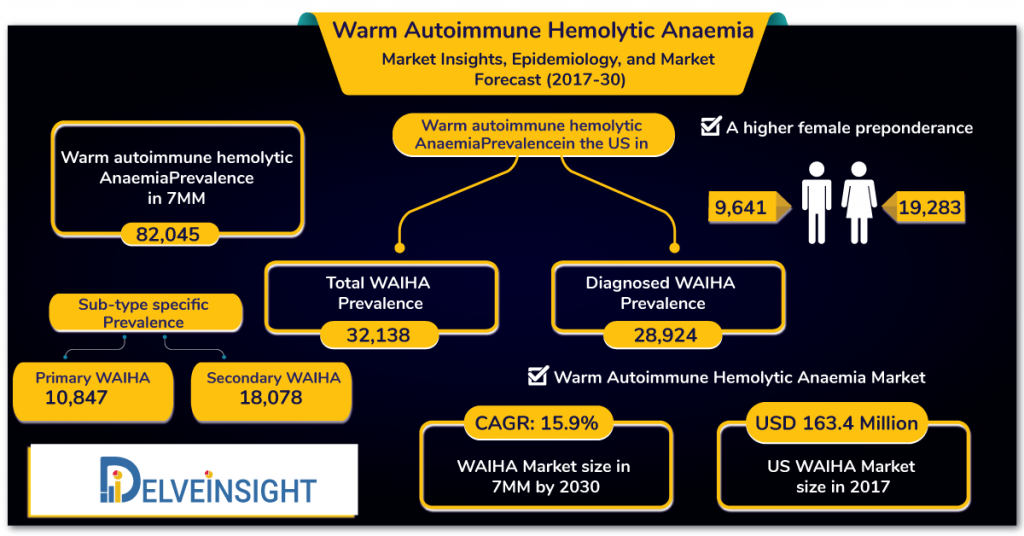
Warm Autoimmune hemolytic Anemia prevalence was estimated the most in the US in 2017 with a total WAIHA prevalence of 32,138. However, total diagnosed Warm Autoimmune hemolytic Anemia prevalence was observed to be around 28,924.
Moreover, a greater preponderance of females was observed in THE US, with 9,641 males and 19,283 females. In terms of type-specific WAIHA prevalence in the US, Primary Warm Autoimmune hemolytic Anemia prevalence was estimated to be around 10,847 cases, whereas Secondary WAIHA prevalence was estimated around 18,078 cases.
Despite being a prevalence of 82,045 in the 7MM in 2017, there is no validated and standard FDA-approved therapeutic option available in the Warm Autoimmune hemolytic Anemia therapy market. It poses a considerable burden on the global healthcare system, with most Warm AIHA patients not been able to achieve a standard cure.
Added to the limited efficacy of currently available therapies, an incomplete understanding of the pathophysiology of WAIHA, the complexity of initiating factors, and a lack of evidence-based standardized therapies, Warm Autoimmune hemolytic Anemia diagnosis, prognosis, and management of continue to be challenging in the present timeline.
However, to redress the current unmet needs in the Warm Autoimmune hemolytic Anemia therapy market, many companies are working to advance the market with several products in the pipeline that shall shift the Warm Autoimmune hemolytic Anemia therapy market positively.
Downloads
Article in PDF
")


