Paragangliomas and Pheochromocytomas Treatment Space Steps into the Precision Therapy Era
Jul 06, 2026
Table of Contents
Summary
- Pheochromocytoma and paraganglioma (PCPG/PPGL) are rare neuroendocrine tumors that arise from chromaffin cells and can occur in the adrenal glands or in extra-adrenal sites such as the thorax, abdomen, pelvis, bladder, and head and neck.
- Surgery remains the only curative option for localized disease, while advanced cases rely on individualized use of alpha and beta blockade, chemotherapy, radionuclide therapy, PRRT, and targeted therapies.
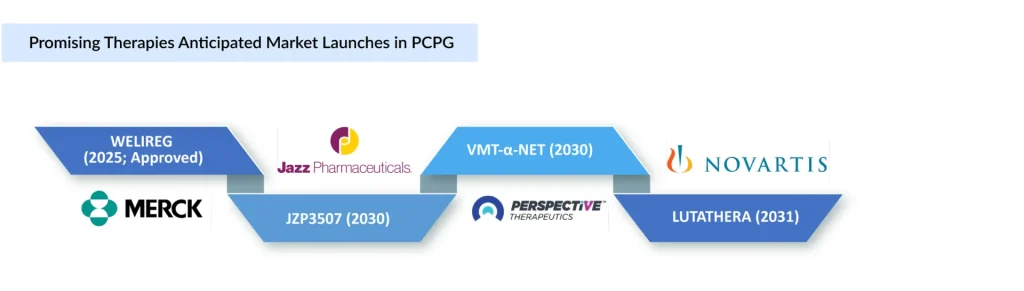
- The approval of Merck’s belzutifan (WELIREG) in May 2025 was a major milestone because it became the first FDA-approved oral therapy for advanced PPGL and added a new precision-based option for eligible patients.
- The pipeline is expanding with radioligand and targeted approaches such as Novartis’ LUTATHERA, Perspective Therapeutics’ VMT-α-NET, and Jazz Pharmaceuticals’ JZP3507, reflecting growing interest in therapies for SSTR2-positive or genetically defined disease.
Pheochromocytoma and paraganglioma (PCPG/PPGL) are rare, heterogeneous neuroendocrine tumors (NETs) that present significant clinical challenges due to their diverse biology and limited treatment options. PCPGs originate from chromaffin cells as adrenal pheochromocytomas or extra-adrenal paragangliomas, which occur in the thorax, abdomen, pelvis, bladder, and head and neck.
Downloads
Click Here To Get the Article in PDF

In 2025, the number of newly diagnosed PCPG cases across the seven major markets (the US, Germany, France, Italy, Spain, the UK, and Japan) reached approximately 4,900, and this figure is expected to rise over the forecast period. These cases are expected to grow at a CAGR of 1.0%. Around three-quarters of all PCPG patients can be assigned to molecular clusters based on mutations.
What are the Critical Unmet Needs?
The growing use of imaging and biochemical testing has led to increased detection of PCPG in recent years. However, despite improved diagnosis, the epidemiological understanding of the disease remains limited, particularly regarding its demographic distribution and long-term disease patterns. This gap becomes even more relevant in metastatic PCPG, where treatment strategies remain largely non-standardized due to the condition’s rarity and limited availability of prospective clinical data.
Advances in molecular profiling have identified three major genetic clusters of PCCs/PGLs, highlighting significant biological heterogeneity and enabling mutation-guided risk stratification and therapeutic decision-making, with surgery remaining the only curative option, while metastatic disease increasingly relies on individualized approaches including CVD/temozolomide chemotherapy, ¹³¹I-MIBG therapy, PRRT with ¹⁷⁷Lu-DOTATATE, and emerging targeted therapies.
|
Key Unmet Need |
Why It Matters |
Strategic Implication |
|
Limited epidemiology |
Detection is rising due to imaging and biochemical testing, but long-term disease and recurrence patterns remain poorly defined. |
Invest in or build disease registries and real-world evidence to estimate true patient burden. |
|
Non-standardized metastatic care |
Metastatic PCPG is rare, heterogeneous, and lacks strong prospective treatment data. |
Opportunity for therapies that define clearer treatment sequencing and clinical positioning. |
|
High molecular heterogeneity |
Mutation-guided treatment remains underdeveloped. Genetic clusters exhibit diverse biology, risk profiles, and treatment sensitivities. |
Prioritize biomarker-led trials and mutation-guided patient selection. |
|
Limited precision therapies |
Molecular profiling is improving, but treatment remains largely individualized. |
Strong opportunity in genetically defined subgroups, especially high-risk SDHB-mutated disease. |
|
Surgery remains the only curative option. |
Unresectable and metastatic disease depend on non-curative systemic or radionuclide approaches. |
New therapies must demonstrate durable disease control and survival relevance. |
|
Weak predictive biomarkers |
Current markers do not reliably predict recurrence, metastasis, or treatment response. |
Biomarker development can improve trial success and support premium positioning. |
|
Rare-disease trial challenges |
Small patient pools limit the feasibility of large prospective studies. |
Global, adaptive, and real-world evidence-based study designs will be essential. |
How Are Malignant/Metastatic PCPGs Treated?
Although most PCPG incident cases remain localized and potentially curable through surgery, a subset progresses to metastatic disease, which is associated with poor prognosis and increased therapeutic complexity. About 15% of PCPGs develop metastatic disease, with factors such as tumor location, Succinate Dehydrogenase Complex Iron Sulfur Subunit B (SDHB) mutations, and other molecular characteristics contributing to aggressive behavior.
For localized disease, radical surgical resection remains the primary curative approach. Successful surgical management, however, depends heavily on careful preoperative pharmacological preparation aimed at controlling hypertension and reducing the risk of intraoperative complications. Standard therapy typically includes alpha blockade followed by beta blockers and other supportive agents when required. Metyrosine (DEMSER), initially approved in the US for the management of pheochromocytomas, continues to retain clinical relevance in preoperative preparation, inoperable disease, and chronic malignant cases, particularly for patients unable to tolerate conventional blockade.
While surgery remains central to management, the therapeutic landscape for advanced PCPG has gradually evolved through the introduction of targeted and radioligand-based therapies. A major development came in 2018 with the US FDA approval of AZEDRA (Iobenguane I-131) for unresectable or metastatic PCPG, marking the first therapy specifically approved for the disease. However, despite its regulatory significance, commercial limitations eventually led to the discontinuation announcement of its production in 2023 (discontinued in Q1 2024), leaving a notable gap in the treatment landscape.
The US approval of Belzutifan (WELIREG) in May 2025 marked another important shift in PCPG management. Six years after acquiring Peloton Therapeutics, Merck is advancing the key asset from that deal rather than letting it sit idle. This new approval applies to patients aged 12 and older with locally advanced, inoperable, or metastatic PPGL. With this, WELIREG becomes the first oral therapy available for advanced forms of PPGL, according to Merck.
As the first and only HIF-2α inhibitor approved for advanced PCPG, the therapy introduced a more targeted, biology-driven approach focused on the hypoxia-inducible factor pathway. Its approval reflects the growing movement toward precision oncology in rare endocrine tumors, particularly as interest in biomarker-guided treatment strategies increases.
The management of PCPGs is advancing through the establishment of dedicated multidisciplinary clinics and the approval of the first targeted systemic therapy. While diagnostic challenges and the rarity of the disease continue to complicate clinical trial execution, the pipeline shows promise, with evolving data on radiopharmaceuticals, a DRD2 antagonist/mitochondrial ClpP activator, an EP4 antagonist, etc.
Among the aforementioned classes, radioligand therapies in PCPG continue to gain importance in the management of metastatic disease. Current guidelines support their use in patients with slowly to moderately progressive metastatic PCPG demonstrating relevant radioisotope uptake. Therapies like LUTATHERA (lutetium Lu 177 dotatate) and [212Pb] VMT-α-NET are being explored in clinical studies, reflecting broader interest in peptide receptor radionuclide therapy for advanced disease.
LUTATHERA is a peptide receptor radionuclide therapy (PRRT) using beta particles. On the other hand, VMT-α-NET is a targeted alpha-particle radiotherapy. Both therapies are designed for SSTR2-positive tumors, a characteristic commonly observed in PCPG. When it comes to radioligand therapies, LUTATHERA is the clinical benchmark, well established and validated, and is likely to remain an important standard for SSTR2-positive disease. VMT-α-NET is the most differentiated radiopharmaceutical, aiming to improve on PRRT through alpha-particle biology and potentially serve patients who relapse after beta-PRRT. VMT-α-NET has received “Fast Track designation” from the US FDA, further reflecting growing interest in its potential clinical role.
When it comes to non-radiopharmaceutical therapies, the PCPG pipeline continues to expand with JZP3507 (ONC206) for advanced or metastatic disease, where treatment options remain limited. JZP3507 is a small-molecule anticancer drug with dual mechanisms: DRD2 (dopamine receptor D2) antagonism and activation of the mitochondrial protease ClpP. These mechanisms induce mitochondrial dysfunction and tumor-cell stress, leading to apoptosis, independent of SSTR2 expression. The potential advantages of this therapy could include no radionuclide administration, the ability to treat tumors irrespective of radionuclide uptake, and the potential for combination with other systemic therapies. If the comparison is based solely on therapeutic modality, JZP3507 is the most mechanistically distinct because it is a non-radiopharmaceutical targeted therapy, although it is much earlier in clinical development and currently has less supporting efficacy evidence in PCPG.
HTL0039732 (NXE0039732) is a novel oral EP4 antagonist developed by Nxera Pharma for cancer treatment. It is being evaluated in a Phase I/IIa trial (NCT05944237; sponsored by Cancer Research UK), including a Phase I/Part B pheochromocytoma cohort, as monotherapy and in combination with atezolizumab. Blocking the EP4 receptor enhances T-cell-mediated anti-tumor immune responses.
The anticipated launch of these emerging therapies is expected to transform the PCPG treatment market landscape in the coming years. As these cutting-edge therapies continue to mature and gain regulatory approval, they are expected to reshape the PCPG market landscape, offering new standards of care and unlocking opportunities for medical innovation and economic growth.
Beyond the Opportunity: The Roadblocks That Could Define Market Success
The pheochromocytoma and paraganglioma (PCPG/PPGL) market is a niche, rare-disease market with a high unmet need. Market growth will be influenced not only by new therapies (e.g., PRRT, alpha-emitting radiopharmaceuticals, and targeted therapies) but also by improvements in diagnosis, referral, and treatment infrastructure.
- Small patient population due to the ultra-rare nature of PCPG/PPGL
- Restricted nuclear medicine infrastructure is limiting access to PRRT and alpha-radiopharmaceuticals
- High treatment and manufacturing costs associated with advanced radiopharmaceutical therapies
- Complex regulatory and reimbursement pathways are delaying market uptake
- Dependence on isotope supply chains and specialized clinical expertise for treatment delivery
Closing Remarks
Despite remaining highly underserved, the PCPG treatment landscape is evolving rapidly, with a robust pipeline spanning next-generation radiopharmaceuticals, targeted therapies, and precision medicine approaches. As multiple assets advance through clinical development, they have the potential to address longstanding unmet needs in metastatic and refractory disease. However, successful market adoption will depend on overcoming barriers such as delayed diagnosis, limited treatment infrastructure, reimbursement challenges, and restricted patient access. Companies that successfully address these commercial and operational challenges alongside clinical differentiation will be best positioned to capture long-term value in the evolving PCPG/PPGL market.

Downloads
Article in PDF



