Ionis’ TRYNGOLZA Approval Raises the Stakes in the Triglyceride-Lowering Race
Jun 29, 2026
Summary
- Over 3 million Americans live with sHTG, including around 1 million high-risk patients with triglycerides ≥880 mg/dL or ≥500 mg/dL plus a history of acute pancreatitis or other comorbidities.
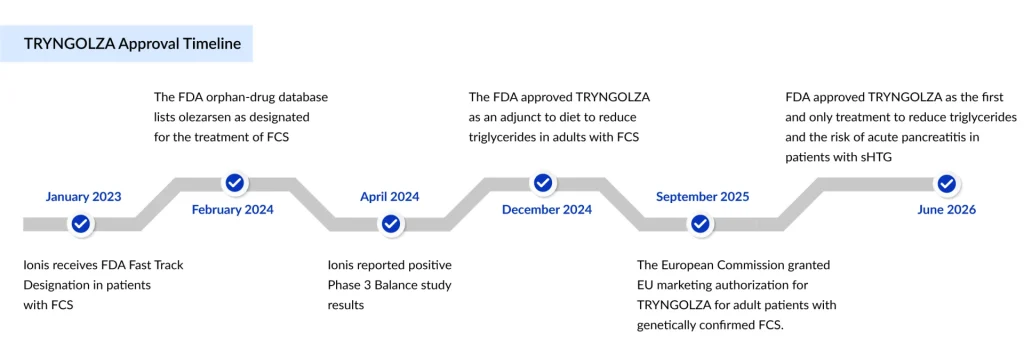
- In June 2026, the FDA approved Ionis’ TRYNGOLZA (already approved for FCS in 2024) as the first and only treatment to reduce triglycerides and the risk of acute pancreatitis in patients with sHTG.
- The TRYNGOLZA approval was based on the data from the Phase 3 CORE and CORE2 trials.
- Key companies such as ArrowHead Pharmaceutical (Plozasiran), 89bio (Pegozafermin), NorthSea Therapeutics (SEFA-1024), and others are evaluating their respective candidates, which will further give competition to TRYNGOLZA once approved.
Severe hypertriglyceridemia (sHTG), defined as fasting triglyceride levels of 500 mg/dL or higher, is far more common than most people realize. More than 3 million people are living with sHTG in the U.S. alone, and roughly 1 million of them fall into the “high-risk” category: triglycerides at or above 880 mg/dL, or 500 mg/dL plus a prior history of acute pancreatitis or other comorbidities. For context, a normal triglyceride reading sits below 150 mg/dL, meaning these patients are walking around with triglyceride levels more than three times, and in many cases, six times, the upper limit of normal.
The clinical stakes are brutal. Acute pancreatitis, the condition that patients are perpetually at risk of, is considered a medical emergency. It causes debilitating abdominal pain that frequently leads to repeated, prolonged hospital stays, can cause permanent organ damage, and can be fatal. Worse, the risk compounds: once a patient has survived one pancreatitis episode, their odds of a repeat attack climb even higher.
Downloads
Click Here To Get the Article in PDF

Despite this, standard-of-care therapies and lifestyle changes, diet, exercise, fibrates, and omega-3s have consistently failed to bring a meaningful share of this population below the 500 mg/dL danger line. From a market-intelligence standpoint, sHTG has long been a textbook case of a prevalent, well-characterized disease with a stubborn treatment gap, exactly the kind of opportunity that draws sustained pharma R&D investment, and exactly what just produced a landmark approval.
From sHTG Treatment Gap to Turning Point: TRYNGOLZA Enters a Crowded but Underserved Market
For years, physicians treating sHTG have leaned on a fairly limited toolkit: fibrates, high-dose omega-3 fatty acids such as icosapent ethyl (marketed as Vascepa/Vazkepa), niacin, and aggressive statin therapy where appropriate, layered on top of strict dietary fat restriction. The problem has never been a lack of options; it’s been a lack of options that actually work for the patients who need them most. Even with multiple agents stacked together, a large proportion of high-risk patients simply cannot get their triglycerides under control, leaving them exposed to recurrent pancreatitis despite doing everything clinicians ask of them.
Ionis Pharmaceuticals’ olezarsen, marketed as TRYNGOLZA, was built to attack the problem at its biological root. It is an RNA-targeted antisense therapy designed to lower the liver’s production of apoC-III, a protein that regulates how triglycerides are cleared from the blood. By suppressing apoC-III, olezarsen restores the activity of lipoprotein lipase, the enzyme responsible for breaking down triglyceride-rich particles, and drives levels down in a way that diet and older drug classes simply cannot match. TRYNGOLZA has already been approved for familial chylomicronemia syndrome treatment, a rare genetic subtype of sHTG, since December 2024.
This latest approval is far bigger in scope: it makes TRYNGOLZA the first and only therapy specifically indicated to reduce both triglycerides and the risk of acute pancreatitis in the broader sHTG population, arriving ahead of its June 30, 2026, PDUFA date and backed by Breakthrough Therapy designation. The data driving the approval, from the Phase 3 CORE and CORE2 trials and published in The New England Journal of Medicine, are striking.
TRYNGOLZA cut fasting triglycerides by up to 72% versus placebo at six months, with 86% of treated patients falling below the critical 500 mg/dL threshold at 12 months. More importantly for patients, acute pancreatitis events dropped by a pooled 85%, with the number needed to treat to prevent one pancreatitis episode falling to just four in the highest-risk subgroup. The drug is self-administered monthly via autoinjector in 50 mg or 80 mg doses and will be available in the U.S. starting in July.
TRYNGOLZA doesn’t have the field to itself, though. Its most direct rival, Arrowhead Pharmaceuticals’ plozasiran (REDEMPLO), is a small interfering RNA (siRNA) therapy that also silences apoC-III and won its own FDA approval for FCS in November 2025, built on strong data from the Phase 3 PALISADE trial.
The two drugs are mechanistically close cousins, and the competitive dynamic mirrors what unfolded in FCS: Ionis got there first in the broader sHTG indication, but plozasiran is right behind it, setting up a head-to-head rivalry in apoC-III suppression that will likely be decided on dosing convenience, safety profile, and real-world adherence as much as on raw efficacy numbers. Older, less targeted options like icosapent ethyl remain on the market too, but neither they nor fibrates can claim what TRYNGOLZA now can: a label that explicitly credits the drug with reducing pancreatitis risk, not just triglyceride numbers on a chart.
The Threats Already Lining Up Behind TRYNGOLZA
First-mover advantage in pharma is rarely a permanent moat, and the sHTG clinical trial pipeline behind TRYNGOLZA is unusually active for a disease this specific. ArrowHead’s Plozasiran is the most immediate threat. Arrowhead is running the SHASTA-3, SHASTA-4, and SHASTA-5 Phase 3 studies specifically to extend its FCS approval into the much larger sHTG population that TRYNGOLZA just captured. Earlier data from the SHASTA-2 and MUIR trials already showed plozasiran delivering deep, durable triglyceride reductions with a dosing schedule of just once every three months, a potential convenience edge over TRYNGOLZA’s monthly injection that could matter a great deal to patients managing a chronic condition for life.
The FDA’s earlier rejection of Ionis’ antisense therapy, volanesorsen, due to thrombocytopenia concerns continues to serve as an important benchmark for the triglyceride-lowering drug class. As next-generation apoC-III–targeting therapies such as TRYNGOLZA and plozasiran expand into broader and more heterogeneous real-world patient populations, close monitoring of platelet counts and liver enzymes remains a key focus for regulators and clinicians.
Meanwhile, Ionis is advancing ION775, an investigational siRNA therapy designed to silence apoC-III for the treatment of sHTG. Engineered for enhanced durability, ION775 has the potential to enable a convenient twice-yearly dosing regimen. The candidate also marks a significant milestone for Ionis, becoming the company’s first siRNA-based therapy to enter clinical development.
For a drug class built on suppressing the same protein through different chemistries, the differentiation battle ahead will increasingly come down to safety margins, dosing intervals, and long-term hepatic data rather than triglyceride percentages alone.
Beyond the apoC-III class itself, other mechanisms are converging on the same patient population. 89bio’s Pegozafermin, an FGF21 analog in development, and earlier-stage candidates targeting ANGPTL3 and related lipid-clearance pathways are also being tracked as emerging sHTG therapies, even though none have yet matched the clinical maturity of olezarsen or plozasiran. Another emerging threat is NorthSea Therapeutics’ SEFA-1024. Though it is a semi-synthetic eicosapentaenoic acid (EPA) derivative, it has the potential to gain significant market share.
What Comes Next: A Market Built for Growth
The commercial runway here is substantial. DelveInsight analysts had already flagged olezarsen as a likely blockbuster well before this approval. Independent market research paints an equally bullish picture for the broader category: the severe hypertriglyceridemia treatment market was valued at roughly USD 1.4 billion in 2023 and is projected to grow significantly by 2036. Those numbers reflect not just pricing power for a first-in-class therapy, but the sheer size of the underlying patient pool still waiting for something that works.
For Ionis, this approval is more than a new product launch; it’s the company’s first fully independent commercial rollout in a prevalent disease, a meaningful step up from its historical focus on rare conditions. With plozasiran’s sHTG trials maturing and several other mechanisms in the wings, TRYNGOLZA’s window of uncontested leadership may be measured in a few short years rather than a decade. But for the millions of patients who have spent years managing triglycerides that diet and older drugs couldn’t touch, that competitive pressure is good news: it means the next wave of innovation in lipid metabolism is already on its way.




