Navigating the Future of Biliary Tract Cancer Treatment: Precision Oncology and Emerging Therapeutic Strategies
Jun 19, 2026
Table of Contents
Summary
- The BTC treatment landscape is shifting from chemotherapy to precision oncology. While gemcitabine-based chemotherapy remains the backbone of first-line and advanced disease treatment, the field has increasingly moved toward biomarker-driven therapy and chemoimmunotherapy.
- Approved targeted therapies are now available for selected biomarker-defined patients. Key examples include FGFR2 inhibitors such as pemigatinib and futibatinib, IDH1 inhibitor ivosidenib, HER2-directed therapies such as trastuzumab deruxtecan and zanidatamab, and tumor-agnostic agents like larotrectinib, entrectinib, dabrafenib + trametinib, and selpercatinib.
- HER2 and FGFR2 are especially important emerging targets.
- The pipeline is expanding quickly. Emerging BTC research includes next-generation combinations, bispecific antibodies, immune-modulating approaches, and novel targets such as KRAS G12C, HER3, B7-H3, B7-H4, CLDN1, FGFR2b, CD47/SIRPα, and TA-MUC1, signaling continued momentum in precision oncology.
BTCs are a group of aggressive malignancies arising from the biliary epithelium, including ICC, ECC, GBC, and ampullary of vater cancer (AVC). These tumors are often diagnosed at advanced stages due to nonspecific symptoms and a lack of screening strategies, resulting in poor prognosis and limited survival.
Downloads
Click Here To Get the Article in PDF

Recent Articles
- New Asundexian Phase III Study Result; Zibotentan/Dapagliflozin Combination Demonstrated Signific...
- Another Feather in the Cap for Xtandi and Keytruda — The Two Main Cancer Drugs
- AstraZeneca’s Imfinzi for Biliary Tract Cancer; FDA Clears Boehringer’s Spesolimab; Novo Nordisk ...
- Eisai Submits Marketing Authorization Application for Tasurgratinib; CHMP Issues Positive Opinion...
- Gilead Sciences’ Sunlenca Approval; FDA Approves Roche’s CD20xCD3 Bispecific Antibody Lunsumio; E...
| Types of BTC | 5-year Survival Rate of BTC | Patient Burden Trends of BTC |
| ICC | ~9–10% | In Western countries, ICC incidence is often higher than ECC |
| ECC | ~10–15% | In East Asian countries like Japan, the proportion of ECC and gallbladder cancer cases is higher |
| GBC | ~20–25% | GBC incidence in the United States has generally been declining over the past two decades |
| AVC | ~45–50% | Overall incidence of BTC in the UK is increasing across all subtypes, with the rise being gradual for AVC compared with more pronounced increases in iCCAs, eCCAs, and GBCs. |
Over the past decade, the treatment paradigm has evolved significantly from reliance on surgery and cytotoxic chemotherapy toward biomarker-driven precision medicine supported by immunotherapy and targeted therapy innovations.
BTC Treatment Enters the Biomarker Era: Beyond Systemic Therapies
According to DelveInsight estimates, there were approximately 65,000 incident cases of BTC across the seven major markets, with nearly 30% of cases occurring in the United States. Japan has a high incidence rate of BTC when compared to Western countries. The BTC patient population is expected to grow over the forecast period, driven by increasing incidence and improved diagnosis rates. Among diagnosed patients, approximately 60–70% eventually progress from early-stage disease to advanced or metastatic BTC, highlighting the substantial burden of disease progression and the need for effective treatment options.
Currently, the relapsed/refractory BTC treatment landscape is largely dominated by therapies, including cytotoxic chemotherapy regimens such as FLOFOX, FOLFIRI, and liposomal irinotecan plus fluorouracil/leucovorin. In recent years, the treatment paradigm has shifted toward biomarker-driven precision medicine, with several targeted therapies receiving regulatory approvals for molecularly defined patient subsets.
These include pemigatinib (PEMAZYRE) by Incyte and futibatinib (LYTGOBI) by Taiho Oncology for patients with FGFR2 fusion-positive cholangiocarcinoma, ivosidenib (TIBSOVO) by Servier Pharmaceuticals for IDH1-mutated cholangiocarcinoma, larotrectinib (VITRAKVI) by Bayer/Loxo Oncology and entrectinib (ROZLYTREK) by Roche/Genentech for NTRK fusion-positive tumors, dabrafenib (TAFINLAR) plus trametinib (MEKINIST) by Novartis for BRAF V600E-mutated tumors, and selpercatinib (RETEVMO) by Eli Lilly for RET fusion-positive solid tumors, including cholangiocarcinoma.
Development in the first-line BTC setting remains relatively limited compared with the relapsed/refractory landscape, with treatment largely centered on chemotherapy-based regimens. Standard first-line BTC treatment options include gemcitabine plus cisplatin (GemCis), along with other recommended regimens such as gemcitabine plus nab-paclitaxel, cisplatin plus gemcitabine plus nab-paclitaxel, capecitabine plus oxaliplatin (CAPEOX), 5-fluorouracil plus oxaliplatin (FOLFOX), and monotherapies including gemcitabine, capecitabine, or 5-fluorouracil for patients unsuitable for combination treatment. Recent advances have been driven primarily by the incorporation of immunotherapy into chemotherapy backbones.
The neoadjuvant/adjuvant BTC treatment market remains largely untapped, with limited approved therapies and significant unmet need. Current management is primarily based on perioperative chemotherapy and adjuvant treatment following surgical resection. Capecitabine (CAPE) is the preferred adjuvant regimen, while other recommended options include 5-fluorouracil plus oxaliplatin (5-FU/OX), capecitabine plus oxaliplatin (CAPEOX), gemcitabine combined with capecitabine, cisplatin, oxaliplatin, or nab-paclitaxel, as well as monotherapy with 5-fluorouracil, capecitabine, or gemcitabine. Despite these chemotherapy-based approaches, no targeted therapies or immunotherapies have been widely established in the perioperative setting, highlighting a substantial opportunity for future therapeutic development.
Systemic Therapy Backbone in Advanced Disease
For patients with unresectable locally advanced or metastatic disease, systemic therapy forms the cornerstone of treatment. Chemotherapy regimens based on gemcitabine combinations remain foundational first-line therapy across global clinical practice. The integration of immunotherapy has significantly changed frontline management, with immune checkpoint inhibitors now incorporated into treatment algorithms. Durvalumab (IMFINZI) represents a major advancement as an approved PD-1 inhibitor used in combination with chemotherapy in the first-line setting, demonstrating meaningful survival benefit. Similarly, pembrolizumab (KEYTRUDA) has expanded treatment options, particularly for biomarker-selected populations, reinforcing the growing role of immunotherapy in BTC management.
How Targeted Therapies are Reshaping the BTC Treatment?
In BTC, drug development is increasingly focused on biomarker-defined patient populations, with the greatest activity concentrated in FGFR2 fusions/rearrangements and IDH1 mutations, particularly in intrahepatic cholangiocarcinoma. Companies such as Incyte, Taiho Oncology, and Servier have played a significant role in validating these targets, making them among the most established biomarker segments in BTC. Beyond these, substantial research activity is focused on HER2 amplification/overexpression, with companies including AstraZeneca and Boehringer Ingelheim actively exploring HER2-targeted strategies. Additional areas of interest include BRAF V600E mutations, NTRK fusions, RET fusions, and KRAS mutations, although these represent relatively smaller patient populations. Immunotherapy development is also focused on biomarkers such as PD-L1 expression, MSI-H/dMMR, and tumor mutational burden (TMB-high) to better identify patients likely to benefit from checkpoint inhibition. More recently, companies have expanded their research efforts toward emerging targets such as CLDN18.2, EGFR, and components of the tumor microenvironment.
FGFR-targeted therapies currently represent one of the most commercially attractive and clinically validated biomarker segments in BTC. Targeted therapies addressing BTC include
- Pemigatinib (PEMAZYRE) and Futibatinib (LYTGOBI), both agents, have demonstrated clinical efficacy in patients with FGFR2 fusion-positive cholangiocarcinoma.
- Zanidatamab (ZIIHERA) and Trastuzumab deruxtecan (ENHERTU) both have favorable clinical efficacy in HER-2 positive BTC, reinforcing HER2 as a promising therapeutic target and supporting continued development for HER2-directed treatment.
- Ivosidenib (TIBSOVO) is approved for patients with IDH1-mutated BTC following prior systemic therapy. Only one IDH therapy.
| HER2 Targeted Approved Therapies | ||||||
| Drug Name | Company Name | ApprovalYear (the US) | Patient Segment | Pivotal Trial | Efficacy Insights | Safety Insights |
| Zanidatamab (ZIIHERA) | Jazz Pharmaceuticals | 2024 | Metastatic HER2-positive (IHC 3+) BTC | HERIZON-BTC-01 (NCT04466891) | ORR: 52%CR: 3.2%PR: 48% | SAE: 53%Discontinuation: 2.5%Dosage interruptions: 41%Dosage reductions: 4% |
| Trastuzumab deruxtecan (ENHERTU) | AstraZeneca and Daiichi Sankyo | 2024 | Metastatic HER2-positive (IHC3+) solid tumors, including BTC | DESTINY-PanTumor02 (NCT04482309), DESTINY-Lung01 (NCT03505710), and DESTINY-CRC02 (NCT04744831) | ORR: 45.5%DoR (months): 2.1 | SAE: 34%FAE: 6.3%Discontinuation: 15%Dose interruptions: 48%Dose reductions: 27% |
| FGFR Targeted Approved Therapies | ||||||
| Drug Name | Company Name | ApprovalYear (Japan) | Patient Segment | Pivotal Trial | Efficacy Insights | Safety Insights |
| Tasurgratinib (TASFYGO) | Eisai | 2024 | Unresectable BTC with FGFR2 gene fusions | Study 201 (NCT04238715) | ORR: 30.2%PR: 30%SD: 49%DCR: 79%Clinical benefit rate: 51% | ≥1 TRAE: 97%≥1 Grade ≥ 3 TRAE: 29%Dose reduction: 54%Treatment interruption: 29%FAE: 6% |
Tumor-agnostic Targeting Expands Therapeutic Opportunities
Tumor-agnostic targeted therapies have expanded treatment options for biomarker-selected patients with BTC. Collectively, these tumor-agnostic approvals emphasize the growing importance of comprehensive genomic profiling and personalized treatment selection in modern BTC management.
- Larotrectinib (VITRAKVI) and entrectinib (ROZLYTREK) are approved for tumors harboring NTRK gene fusions, irrespective of tumor origin, including BTC.
- Dabrafenib + trametinib (TAFINLAR + MEKINIST) provides an approved targeted treatment option for patients with BRAF V600E-mutated disease.
- Selpercatinib (RETEVMO) is an approved RET inhibitor indicated for patients with RET fusion-positive biliary tract cancers.
| Genomic Alterations and Corresponding Targeted Therapeutic Strategies for BTCs | |||
| Molecular Alteration | Actionable Target | Available Drugs | Company Name |
| IDH1 mutation | IDH inhibitors | Ivosidenib (TIBSOVO) | Agios Pharmaceuticals/Servier Pharmaceuticals |
| RET gene fusion | Kinase inhibitors | Selpercatinib (RETEVMO) | Eli Lilly |
| FGFR2 | FGFR inhibitors | Futibatinib (LYTGOBI) | Taiho |
| Pemigatinib (PEMAZYRE) | Incyte | ||
| TMB-H | ICIs | Pembrolizumab (KEYTRUDA) | Merck |
| Durvalumab (IMFINZI) | AstraZeneca | ||
| BRAF V600E mutation | BRAF inhibitors | Dabrafenib (TAFINLAR) + Trametinib (MEKINIST) | Novartis |
| MSI-H/dMMR | Immune checkpoint inhibitors | Pembrolizumab (KEYTRUDA) | Merck |
| Durvalumab (IMFINZI) | AstraZeneca | ||
| NTRK gene fusion | NTRK inhibitors | Entrectinib (ROZLYTREK) | Roche/Genentech |
| Larotrectinib (VITRAKVI) | Bayer/Loxo Oncology | ||
Current Unmet Needs
A significant unmet need remains in BTC, as many biomarker-defined patient populations lack approved targeted therapies beyond established segments such as HER2, FGFR2, and IDH1. Despite advances in biomarker-driven therapy for BTC, several genomic alterations remain largely untapped or lack approved targeted treatment options. Common alterations such as CDKN2A/B, TP53, ARID1A, KRAS, SMAD4, and PBRM1, along with less frequent but actionable biomarkers including BRAF, NTRK1, RET fusions, MSI-H/dMMR, and TMB-H, represent significant opportunities for therapeutic development. Expanding effective targeted and biomarker-guided treatment strategies for these patient subsets remains a key unmet need in BTC.
Furthermore, apart from immune checkpoint inhibitor (ICI)-based combinations, there are limited approved biomarker-directed therapies in the first-line setting, highlighting a significant need for novel targeted treatments that can improve outcomes for these patient populations.
Advancing the Frontier: Momentum in BTC Drug Development
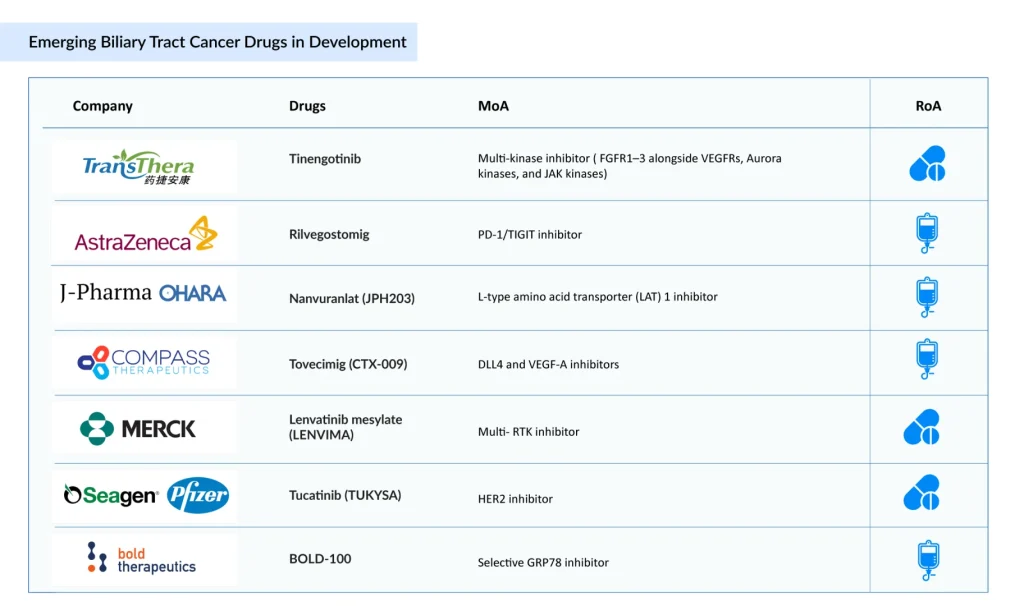
The BTC pipeline is expanding across a diverse range of emerging biomarkers and targets, including LAT1, DLL4/VEGF-A, GRP78, CK2, HER3, KRAS G12C, CD47/SIRPα, CLDN1, FGFR2b, B7-H3, B7-H4, and TA-MUC1. This growing biomarker diversity highlights the increasing role of precision oncology and immuno-oncology in BTC development.
Persistent Need for Effective Post-progression Therapies
Tinengotinib (TransThera Sciences) and Nanvuranlat (J-Pharma/OHARA Pharmaceutical) are in Phase III development for previously treated advanced BTC patients.
Next-generation Frontline Combination Strategies
The frontline BTC landscape is evolving with novel antibody-based therapies, including Zanidatamab (ZIIHERA) plus chemotherapy, trastuzumab deruxtecan (ENHERTU) plus rilvegostomig, and rilvegostomig with chemotherapy, all being evaluated in Phase III studies.
Immune Modulation Approaches
Additional innovative therapies in BTC include tovecimig, a DLL4/VEGF-A bispecific antibody being evaluated in combination regimens across first- and later-line settings, and silmitasertib (CX-4945), a Casein Kinase 2 (CK2) inhibitor in Phase II development for cholangiocarcinoma.
Novel Therapeutic Modalities and Platform Innovation
Novel BTC therapies under development include VG161, an oncolytic virus therapy, BOLD-100, a GRP78 inhibitor combined with FOLFOX, and tucatinib (TUKYSA), an oral HER2-targeted tyrosine kinase inhibitor, all being evaluated in Phase II studies.
Unlocking the Potential of Untapped Early-stage BTC Market Expansion
In early-stage BTC, surgical resection remains the only potentially curative treatment and the standard approach. Among emerging therapies, rilvegostomig, a PD-1/TIGIT bispecific antibody developed by AstraZeneca and Compugen, is being evaluated in the Phase III ARTEMIDE-Biliary02 trial. If successful, it could be launched around 2030, providing a novel immunotherapy option for BTC.
The BTC development landscape is witnessing growing interest from a diverse group of biotechnology and pharmaceutical companies, reflecting the increasing recognition of the disease’s unmet medical need and commercial potential.
Conclusion
The BTC treatment landscape has evolved from a predominantly chemotherapy-based approach to one increasingly driven by chemoimmunotherapy and biomarker-targeted therapies, with approved options for FGFR2, IDH1, HER2, BRAF, NTRK, and RET-altered tumors. The BTC clinical trial pipeline continues to expand with novel immunotherapies, bispecific antibodies, and next-generation targeted agents. However, significant unmet needs remain, particularly for patients without actionable mutations and in the neoadjuvant/adjuvant setting, where treatment options are limited, and recurrence rates remain high. Looking ahead, untapped biomarker segments such as KRAS G12C, HER3, B7-H3, B7-H4, CLDN1, FGFR2b, c-MET, and CD47/SIRPα present promising opportunities to broaden precision medicine approaches and drive the next wave of innovation in BTC.

Downloads
Article in PDF
Recent Articles
- Biliary Tract Cancer: Emerging Players in the Market Transforming the Treatment Landscape
- Gilead Sciences’ Sunlenca Approval; FDA Approves Roche’s CD20xCD3 Bispecific Antibody Lunsumio; E...
- Gastrointestinal Cancers: Exploring the Range of Digestive Tract Malignancies
- AstraZeneca’s Imfinzi for Biliary Tract Cancer; FDA Clears Boehringer’s Spesolimab; Novo Nordisk ...
- New Asundexian Phase III Study Result; Zibotentan/Dapagliflozin Combination Demonstrated Signific...



