Fusion Biopsy: The Next Generation of Prostate Cancer Detection
Jun 24, 2026
Table of Contents
Prostate cancer remains the second most common malignancy diagnosed in men worldwide, with global incidence now exceeding 1.4 million new prostate cancer cases a year. For decades, the diagnostic pathway leaned on a blunt instrument: a 12-core systematic biopsy taken largely by anatomical guesswork. That era is closing. Fusion biopsy, which overlays high-resolution MRI data onto real-time ultrasound to guide the needle directly into suspicious tissue, has moved from a niche academic technique to a standard-of-care diagnostic in leading urology centers.
The numbers tell the story plainly. In a large 1,229-patient cohort stratified by PI-RADS score, MRI-ultrasound fusion biopsy detected clinically significant prostate cancer in 50% of cases compared with 35.3% for systematic biopsy alone, with detection climbing to 95.6% for the highest-suspicion PI-RADS 5 lesions. A separate meta-analysis of more than 3,400 cases found fusion-guided biopsy was 22% more likely to catch clinically significant disease than the systematic approach (RR=1.22, P<0.01). And it isn’t just about catching more cancer, it’s about catching the right cancer, since fusion techniques consistently reduce overdiagnosis of low-grade, clinically insignificant disease that doesn’t need treatment.
Downloads
Click Here To Get the Article in PDF

Recent Articles
- Clover’s SCB-1019 RSV Revaccination Study Clears U.S. IND; FDA Approves AMVUTTRA for ATTR-CM CV R...
- Hanmi Pharmaceutical and Eli Lilly and Company Join Forces to Advance Sonefpeglutide Development;...
- VARON’s New VP Series Portable Oxygen Concentrator; Biostrap’s Wrist-Worn Digital Health Monitori...
- A Quick Recap from ASCO GU 2023: Prostate and Urothelial Cancer Highlights
- Now, Nanoparticles for Cancer Treatment
This is the essence of fusion biopsy’s promise: bridging the gap between what imaging can see and what a needle can reach. MRI identifies the lesion; ultrasound provides the real-time, in-procedure visualization; fusion software fuses the two into a single navigable map. The result is a diagnostic workflow that trades blind sampling for targeted precision, and the global market is responding.
Clinical Advantages Driving Adoption
The clearest argument for fusion biopsy is diagnostic yield where it matters most. Across multiple large cohort studies, fusion-guided sampling consistently outperforms systematic biopsy at identifying clinically significant prostate cancer (csPCa), the disease that actually threatens a patient’s life, while simultaneously detecting fewer indolent, low-grade tumors that would otherwise trigger unnecessary treatment. One propensity-matched study found fusion biopsy detected csPCa in 58% of patients versus 41% with conventional biopsy, a gap wide enough to change clinical decision-making at the point of diagnosis.
This precision translates directly into a better experience for patients. Because fusion biopsy targets specific lesions rather than blanketing the gland with cores, many protocols require fewer needle passes, which in turn lowers the risk of bleeding, infection, and the urinary side effects historically associated with prostate sampling. The growing shift toward transperineal fusion approaches compounds this advantage further, as the route avoids passing the needle through rectal flora altogether, meaningfully cutting sepsis risk compared to the transrectal pathway.
Fusion biopsy is also reshaping who gets re-biopsied and why. For men with a prior negative systematic biopsy but persistently elevated PSA, a frustratingly common clinical scenario, fusion-guided rebiopsy can locate and sample lesions in the anterior and apical zones that conventional sextant or 12-core templates routinely miss. This single capability addresses one of urology’s longest-standing diagnostic blind spots, and it explains why professional bodies like the American Urological Association and the National Comprehensive Cancer Network have increasingly woven multiparametric MRI and targeted biopsy into their guidance for high-risk and biopsy-naïve patients alike.
Finally, there’s a quieter but equally important advantage: better risk stratification feeds directly into better treatment decisions. A biopsy that more accurately reflects the true grade of a tumor reduces the chance of a Gleason score upgrade at final prostatectomy pathology, a mismatch that, when it happens with systematic biopsy alone, can mean a patient was initially steered toward the wrong management pathway, whether that’s active surveillance when surgery was warranted, or vice versa.
Technological Evolution and Integration
Fusion biopsy has evolved considerably from its earliest “cognitive fusion” form, where a radiologist’s MRI read was mentally overlaid onto a live ultrasound image by the performing urologist, a method entirely dependent on operator skill and prone to targeting error. Software-based fusion platforms changed that equation by digitally registering pre-acquired MRI volumes onto real-time ultrasound, correcting for prostate movement and deformation during the procedure itself. This software-fusion category remains the dominant technique in the market today, prized for combining strong accuracy with workflow efficiency that doesn’t require an MRI suite to be present during the biopsy itself.
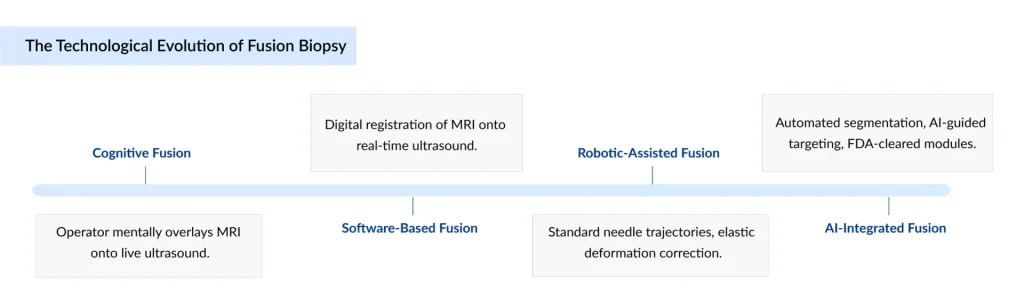
A parallel evolution has occurred in hardware. Robotic-assisted fusion platforms now offer steadier, more reproducible needle trajectories than the freehand technique, while elastic image-registration algorithms increasingly account for the gland’s natural shifting and compression during a procedure, a long-standing source of targeting drift. At the same time, in-bore MRI fusion, where biopsy is performed inside the MRI scanner itself for maximal real-time accuracy, continues to carve out a role for complex or previously inconclusive cases, even as it remains more resource-intensive than ultrasound-based fusion.
Integration is the throughline connecting all of this. Modern fusion platforms are being built to talk to hospital PACS systems, automate 3D prostate contouring, and shorten the radiologist-to-urologist handoff that used to introduce delay and miscommunication into the diagnostic pathway. Vendors are explicitly marketing connected radiology-urology workflows rather than standalone devices, recognizing that a biopsy system’s clinical value is now inseparable from how cleanly it fits into the broader diagnostic ecosystem.
Role of AI in Fusion Biopsy
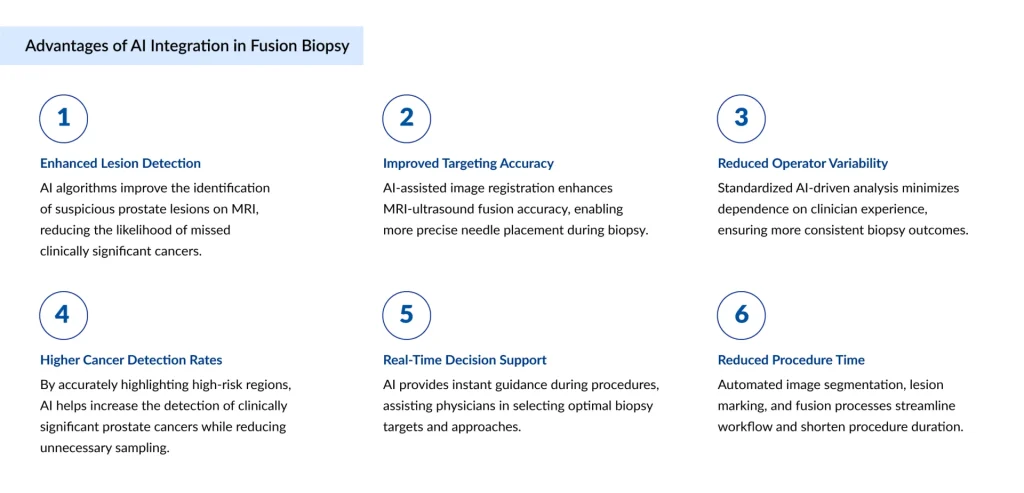
Artificial intelligence has become the defining differentiator in the next generation of fusion biopsy platforms, and its footprint starts before the patient ever reaches the procedure room. AI-powered segmentation tools can now automatically delineate the prostate capsule and flag suspicious regions on MRI in seconds, a task that previously required a radiologist to manually trace gland boundaries slice by slice. This isn’t a marginal convenience: faster, more consistent segmentation directly improves the registration accuracy that the entire fusion process depends on.
Inside the procedure itself, AI is increasingly handling the real-time mechanics of targeting. Algorithms now assist with needle trajectory planning and compensate computationally for the deformation a prostate undergoes when an ultrasound probe is introduced, historically one of the most stubborn sources of inaccuracy in fusion biopsy. Recent regulatory milestones underscore how fast this is moving: in early 2026, KOELIS received FDA 510(k) clearance for an AI-powered lesion-targeting module on its Trinity platform, marking the first such clearance for an AI-augmented MRI-ultrasound fusion biopsy system and signaling that AI-assisted targeting is moving from research interest to commercially deployed, regulator-approved capability.
AI is also tackling the long-standing skill gap between high-volume academic centers and lower-volume community practices. Learning-curve data shows that csPCa detection rates with fusion biopsy can rise from roughly 35% to 60% as a clinical team gains experience over several years, a steep curve that disadvantages smaller centers. By automating segmentation, standardizing lesion scoring, and guiding less-experienced operators through optimal needle placement, AI tools are effectively compressing that learning curve, helping community urology practices approach outcomes once reserved for specialized academic institutions.
Looking ahead, the frontier is shifting toward predictive and multimodal AI, models that don’t just locate a lesion but help estimate its likely grade by fusing imaging features with PSA kinetics, prior biopsy history, and increasingly, genomic risk scores. Pilot programs combining fusion biopsy with genomic risk profiling are already underway at academic medical centers, hinting at a near future where the biopsy itself becomes one data input among several feeding a single, AI-synthesized risk picture for each patient.
Fusion Biopsy Market Momentum and Global Outlook
The commercial trajectory of fusion biopsy reflects its clinical momentum. DelveInsight forecasts place the global fusion biopsy market at USD 800 million in 2025, with projections converging around USD 1.5 billion by 2034, representing a compound annual growth rate generally estimated at 7.4%. Within the product segment of the fusion biopsy market, the equipment category is contributing to 69% of total market revenue in 2025, due to its central importance in enabling accurate, image-guided diagnostic procedures.
Geographically, North America continues to lead, commanding the largest regional share, cited 43% of global revenue, on the back of dense screening infrastructure, established Medicare and private insurer reimbursement codes specific to fusion biopsy procedures, and strong clinical guideline backing from the AUA and NCCN. Asia-Pacific is consistently flagged as the fastest-growing region, propelled by rising prostate cancer incidence tied to aging populations, expanding hospital imaging infrastructure, and growing screening awareness across China, Japan, and India.
Care setting is shifting, too. While hospitals still account for the majority of procedure volume, ambulatory surgical centers are emerging as the fastest-growing end-user segment, a trend consistent with fusion biopsy’s profile as a shorter, often better-tolerated outpatient procedure compared with older biopsy approaches. On the technology side, the transperineal route is broadly projected to outgrow the long-dominant transrectal approach, driven by its lower infection profile and improving anterior-zone accessibility, even as transrectal techniques retain the larger installed base for now.
Competitively, the field includes established imaging giants, Koninklijke Philips N.V., KOELIS S.A., innoMedicus Ltd., Siemens Healthineers AG, MedCom GmbH, Exact Imaging Inc., Focal Healthcare Inc., Biobot Surgical Pte. Ltd., Esaote S.p.A., GE HealthCare Technologies Inc., Hitachi Medical Systems (Hitachi, Ltd.), Canon Medical Systems Corporation, BK Medical Holding Company, Inc., Eigen, Inc., UroMedTech GmbH, D&K Technologies Pvt. Ltd., alongside specialized fusion-platform innovators like KOELIS, Eigen, Exact Imaging, Biobot Surgical, and BiopSee.
Recent moves, including KOELIS’s AI-targeting FDA clearance and its partnership with Bot Image for automated 3D lesion contouring, illustrate where competitive differentiation is heading: not toward new hardware alone, but toward smarter, faster, more autonomous software layered on top of it. As reimbursement structures mature and AI-assisted platforms continue clearing regulatory bars, fusion biopsy looks set to shift from “advanced option” to default standard across a widening share of the world’s urology practices.
Fusion Biospy Shaping the Future of Prostate Cancer Care
Fusion biopsy represents a paradigm shift in prostate cancer diagnostics, aligning with the broader movement toward precision medicine. By enabling more accurate detection and risk stratification, it supports tailored treatment strategies that can improve patient outcomes while minimizing unnecessary interventions.
Looking ahead, fusion biopsy is expected to play a central role in active surveillance programs, where precise and repeatable targeting of lesions is critical. Patients with low-risk prostate cancer can be monitored more effectively, reducing the likelihood of disease progression going undetected while avoiding aggressive treatments that may impact quality of life. This shift toward surveillance-driven care models is particularly relevant as healthcare systems aim to balance clinical outcomes with cost-efficiency.
Moreover, the integration of fusion biopsy with genomic profiling and biomarker-driven diagnostics is set to further refine prostate cancer management. Combining imaging precision with molecular insights can help clinicians better understand tumor biology, enabling more personalized therapeutic decisions. This convergence of technologies supports the transition from a one-size-fits-all approach to a more nuanced, patient-centric care pathway.
From a healthcare systems perspective, the adoption of fusion biopsy also has implications for resource optimization and long-term cost savings. By reducing repeat biopsies, minimizing overtreatment, and improving diagnostic confidence, hospitals and clinics can enhance operational efficiency while delivering higher-quality care. As reimbursement models increasingly favor value-based care, technologies like fusion biopsy are well-positioned to gain stronger clinical and economic validation.

Downloads
Article in PDF
Recent Articles
- Biogen-Eisai’s Aduhelm; Quidel acquires Ortho Clinical Diagnostics; Accutar Biotechnology’s...
- 8 Key Applications of Radioligand Therapies in Healthcare
- Accutar’s Phase I clinical trial for AC0176; Bio-Thera’s cancer drug, BAT6005; Nykode...
- Bristol Myers’ Opdivo combo Opdualag for Melanoma; Biogen’s Aduhelm; Marinus’ Ztalmy for CDKL-5 D...
- Nanoscope’s MCO-010 Begins FDA Rolling Submission for Retinitis Pigmentosa; Bayer’s KERENDIA Appr...



