The Oral GLP-1 Revolution: How Pill-Based Drugs Are Reshaping the Obesity Treatment Space
Jun 15, 2026
Table of Contents
Summary
- The obesity drug landscape is shifting from injectable GLP-1s to oral pill-based treatments, marking a major turning point in pharmacotherapy.
- Two oral GLP-1s have now received FDA approval: Novo Nordisk’s WEGOVY pill (December 2025) and Eli Lilly’s FOUNDAYO (April 2026).
- Several companies, such as Pfizer (PF-07976016), Regor Therapeutics (RGT-075), AstraZeneca (AZD5004), and others, are also evaluating their oral GLP-1 candidates to give competition to Novo and Eli Lilly.
The era of needle-only obesity treatment is officially over. After years of blockbuster injectable drugs dominating headlines, and medicine cabinets, the obesity pharmacotherapy landscape is being flipped on its head by a new class of pill-based GLP-1 treatments. From FDA-approved oral semaglutide to Eli Lilly’s freshly greenlit FOUNDAYO, the race to put a once-weekly injection into a once-daily tablet has crossed the finish line, and it’s only just getting started.
Downloads
Click Here To Get the Article in PDF

Recent Articles
- Redefining Liver Disease in the Metabolic Era: From NASH to MASH and the Rise of Obesity‐targeted...
- Intensity Therapeutics Publishes Compelling Clinical Data for INT230-6 in Advanced Cancers; UCB W...
- WEGOVY: A Leader in the Obesity and Weight Loss Treatment
- Novo Nordisk Seeks FDA Approval for CagriSema; EU Approves Subcutaneous Self-administration of SA...
- Hengrui Pharma Encounters FDA Regulatory Hurdle for Camrelizumab–Rivoceranib; Kailera Therapeutic...
For patients who’ve avoided treatment due to needle phobia, cost barriers, or simply the inconvenience of cold-chain logistics, this moment represents a seismic shift. And for the pharmaceutical giants behind WEGOVY and ZEPBOUND, two of the best-selling drugs in modern history, the oral revolution is both their biggest opportunity and their greatest competitive threat.
Setting the Scene: Why the Injectable Era Had a Ceiling
The anti-obesity treatment market has become synonymous with one of the most closely watched rivalries in modern pharmaceuticals: Novo Nordisk versus Eli Lilly. Novo Nordisk effectively created the modern obesity drug market with the launch of WEGOVY (semaglutide) in 2021, transforming obesity management from a lifestyle-focused intervention into a highly effective pharmacological treatment option. The therapy generated approximately USD 8 billion in U.S. sales in 2025 alone, while the company continued to strengthen its position through geographic expansion and label enhancements. By the end of 2025, WEGOVY was available in 52 countries worldwide, nearly doubling its global footprint, with additional launches planned for 2026, subject to regulatory approvals.
The competitive landscape intensified in 2023 when Eli Lilly entered the market with a differentiated clinical profile. Tirzepatide, a dual GIP/GLP-1 receptor agonist, demonstrated superior efficacy to semaglutide in a landmark head-to-head trial, with patients receiving ZEPBOUND losing an average of 50 pounds over 72 weeks compared with 33 pounds among WEGOVY-treated patients. This compelling efficacy advantage significantly influenced prescribing patterns and patient preferences. As a result, ZEPBOUND generated approximately USD 13.4 billion in U.S. sales during 2025, surpassing expectations and accelerating Lilly’s market share gains.
Together, these breakthrough GLP-1-based therapies demonstrated unprecedented efficacy, enabling patients to achieve 15–21% body weight reduction, results that were previously attainable primarily through bariatric surgery. Despite their remarkable clinical success, several real-world barriers have constrained broader adoption. Weekly self-injections remain a deterrent for many patients due to needle aversion, while refrigerated storage requirements create logistical challenges, particularly in rural and resource-limited settings.
Cost has emerged as another major hurdle, with monthly treatment expenses typically ranging between USD 1,000 and USD 1,400 without insurance coverage. Persistent supply shortages of both WEGOVY and ZEPBOUND have further widened the treatment gap as manufacturers struggled to keep pace with overwhelming demand. Consequently, although obesity affects hundreds of millions of people globally, GLP-1 therapies currently reach only a small fraction of eligible patients, underscoring the substantial unmet need for more convenient, scalable, and accessible treatment options.
According to Sadaf Javed, an endocrinology and metabolic disorders expert at DelveInsight, Eli Lilly is currently positioned as the frontrunner in the GLP-1-based obesity market, supported by its clinical differentiation, robust intellectual property protection, and expanding commercial reach. Nevertheless, the obesity market remains highly dynamic, and the competitive story is far from over. Novo Nordisk continues to invest aggressively in its next-generation obesity pipeline and lifecycle management strategies, setting the stage for an increasingly intense battle for leadership in one of the fastest-growing pharmaceutical markets globally.
Under the Hood: The Science That Made Oral GLP-1 Possible
Getting a GLP-1 peptide into pill form isn’t trivial science. These are large, fragile protein molecules that the digestive system would ordinarily destroy before they could reach the bloodstream. The oral semaglutide solution involved co-formulating the peptide with SNAC (sodium N-[8-(2-hydroxybenzoyl)aminocaprylate), an absorption enhancer that protects semaglutide from enzymatic breakdown in the stomach and facilitates transcellular absorption through the stomach wall. The result is a bioavailability profile sufficient to drive clinically meaningful weight loss, something the scientific community long considered impossible for peptide-based GLP-1s.
The Historic WEGOVY Pill Approval
On December 22, 2025, the FDA made history. It approved the WEGOVY pill (oral semaglutide 25 mg), the world’s first oral GLP-1 receptor agonist approved for chronic weight management in the United States. Novo Nordisk launched it in early January 2026, and the obesity market hasn’t looked back.
The approval was based on the OASIS 4 Phase 3 trial, a 64-week study involving 307 adults with obesity or overweight. The results were striking: participants on oral semaglutide achieved a mean weight loss of 13.6%, compared to just 2.2% on placebo. When patients stayed on treatment for the full duration, that number climbed to 16.6%, essentially matching the weight loss performance of injectable WEGOVY 2.4 mg.
The WEGOVY pill isn’t just indicated for weight loss. Like its injectable counterpart, it also carries approval to reduce the risk of major adverse cardiovascular events (MACE), including cardiovascular death, heart attack, and stroke, in adults with established heart disease and obesity or overweight. That cardiovascular indication is a clinically and commercially powerful differentiator.
The pill is available in strengths of 1.5 mg, 4 mg, 9 mg, and 25 mg, with a starting dose of 1.5 mg. Novo Nordisk priced it at a self-pay entry point of $149/month for the lowest dose, making it the most affordable GLP-1 obesity treatment to date.
Eli Lilly Fires Back with FOUNDAYO
Novo Nordisk’s head start didn’t last long. On April 1, 2026, the FDA approved Eli Lilly’s FOUNDAYO (orforglipron), the second oral GLP-1 approved for obesity, and arguably the one with the more patient-friendly convenience profile.
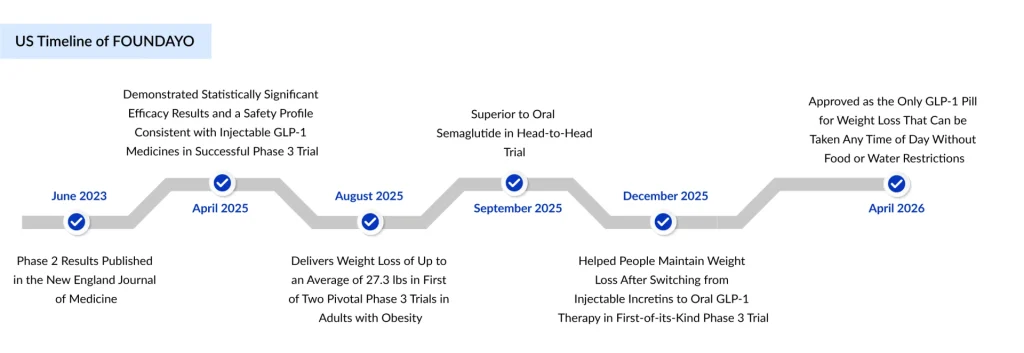
FOUNDAYO is a small-molecule, non-peptide GLP-1 receptor agonist. This is a critical technical distinction. The WEGOVY pill is a peptide-based molecule (semaglutide) that requires an absorption enhancer (SNAC) and must be taken fasting, 30 minutes before eating or drinking anything other than water. FOUNDAYO, by contrast, can be taken at any time of day, with or without food, with or without water. No fasting. No timing rules. Just take it. This pharmacological advantage could prove decisive in the real-world adherence battle.
Clinically, the ATTAIN Phase 3 program showed that orforglipron at its highest dose delivered a mean weight loss of 12.4% over 72 weeks, slightly less than the WEGOVY pill’s 13.6% at 64 weeks, but with a broader, more diverse patient population of over 3,000 participants. More than 54.6% of participants achieved ≥10% weight loss, alongside meaningful improvements in cardiometabolic markers, including blood pressure, waist circumference, and lipid levels.
Eli Lilly priced FOUNDAYO comparably to the WEGOVY pill, with self-pay access starting at $149/month for the lowest dose, eligible commercial insurance patients paying as low as $25/month with savings cards, and Medicare Part D patients expected to access it for $50/month beginning July 1, 2026.
The Oral GLP-1 Pipeline: More Challengers Are Coming
The obesity drug pipeline is one of the most dynamic and rapidly evolving areas in modern medicine, with more than 100 candidates in development targeting diverse physiological pathways. While the currently approved GLP-1 therapies have transformed obesity management, they represent only the first wave of innovation. A robust pipeline of oral GLP-1 agents and next-generation therapies with complementary mechanisms is advancing swiftly, intensifying competition and expanding future treatment possibilities.
Pfizer’s PF-07976016
Pfizer was once the most aggressive challenger in the oral GLP-1 race. Its small-molecule candidate danuglipron showed promising efficacy, with placebo-adjusted weight reductions of 8–13% in Phase 2b trials. But the path to approval was rocky. High gastrointestinal discontinuation rates exceeding 50% across all doses, combined with liver safety signals in early studies, ultimately led Pfizer to discontinue danuglipron’s development in April 2025. The company, however, has not abandoned the space. It is continuing the development of an oral GIPR antagonist candidate (PF-07976016) in Phase 2, and maintains an earlier-stage obesity pipeline.
Regor Therapeutics’ RGT-075
RGT-075 is a once-daily oral small-molecule GLP-1 receptor full agonist being developed by Regor for the treatment of metabolic disorders such as type 2 diabetes mellitus, obesity, and overweight conditions linked with weight-related comorbidities. The candidate has previously advanced through Phase IIa clinical evaluation in obese patients, as well as Phase I single ascending dose (SAD) studies in healthy volunteers and multiple ascending dose (MAD) studies in diabetic patients. Results from these studies have shown that RGT-075 is generally safe and well tolerated, while preliminary efficacy data suggest its therapeutic potential may be comparable to currently approved peptide-based GLP-1 therapies.
AstraZeneca’s AZD5004
AstraZeneca is developing its own oral small-molecule GLP-1RA, AZD5004, currently in earlier-stage trials. Given the commercial scale of the obesity market, AstraZeneca is one of several large pharma players betting that the oral delivery format will be the dominant paradigm within a decade.
How Oral GLP-1s Will Challenge WEGOVY and ZEPBOUND Dominance?
Make no mistake: injectable Novo’s WEGOVY and Eli Lilly’s ZEPBOUND still hold significant clinical advantages. Injectable WEGOVY achieves up to 15–17% weight loss on average, and ZEPBOUND has demonstrated up to 22.5% weight loss at the highest doses. Retatrutide’s near-29% weight loss figures are in a league of their own. On pure efficacy, the injectables still lead.
But markets don’t run on peak efficacy alone. They run on access, adherence, convenience, price, and patient preference, and on every one of those metrics, oral GLP-1s are poised to win large segments of the market.
The Needle-Averse Market is Massive
A survey of over 1,000 adults living with obesity found that 71% would prefer a daily pill over a weekly injection when choosing a prescription weight-loss medication. This is an enormous addressable patient population that has either never started injectable therapy or discontinued it. Novo Nordisk specifically identified demographics, including men and younger individuals, as being less inclined to use injectables, groups that oral options are particularly likely to engage.
Pricing Pressure Accelerates Adoption
At $149/month self-pay for the starter dose, oral GLP-1s enter the market at a materially more accessible price point than injectable WEGOVY (which retails at $1,349/month before discounts). Even if clinical responders eventually titrate to higher, and more expensive, oral doses, the entry-level affordability lowers the initiation threshold dramatically, especially for patients without robust insurance coverage.
Cold-Chain Logistics Are Eliminated
Oral pills require no refrigeration. This might seem like a minor operational detail in the United States, but globally it is transformative. In markets across Asia, Africa, Latin America, and parts of Eastern Europe where cold-chain infrastructure is unreliable, oral GLP-1s have the potential to unlock access to hundreds of millions of patients who could never have reliably received injectable therapy.
Adherence and Convenience Drive Long-Term Market Share
Obesity is a chronic condition requiring indefinite treatment. The therapy that patients stay on longest wins in the market. Daily oral dosing, particularly FOUNDAYO’s restriction-free “take it anytime” convenience, may prove to have significantly better long-term adherence profiles than weekly injections, which require patients to self-inject, rotate injection sites, and manage sharps disposal.
The Oral-to-Injectable Bridge
Interestingly, oral GLP-1s may not always cannibalize injectable therapy; they may serve as an on-ramp to it. Orforglipron’s Phase 3 ATTAIN-MAINTAIN trial specifically demonstrated that patients could successfully transition from injectable GLP-1s to orforglipron and maintain their weight loss. This creates a clinical flow where patients initiate on oral therapy, stabilize, and either remain on pills or step up to higher-efficacy injectables based on their clinical needs, a tiered treatment model that expands the overall market rather than simply redistributing it.
Market Share Projections
Novo Nordisk itself forecasts that oral weight-loss drugs will capture more than one-third of the total GLP-1 market by 2030. The GLP-1 obesity market overall is projected to grow dramatically in 2026 and beyond, driven by reduced prices, expanded Medicare and Medicaid coverage, and the newfound accessibility of oral options. With GLP-1 penetration still at roughly 2% of the obese population globally, even a modest increase in uptake represents enormous commercial expansion.
The Road Ahead: Oral Dominance Is Not Inevitable
Despite the growing commercial momentum surrounding oral GLP-1 therapies, the segment continues to face several important challenges that may affect long-term adoption and market expansion. One of the most significant concerns is the efficacy gap between oral and injectable GLP-1 treatments. Even in favorable head-to-head comparisons, oral GLP-1 therapies have demonstrated weight loss outcomes of approximately 12–16%, while leading injectable therapies consistently deliver around 17–22% or higher. For patients with severe obesity or obesity-associated comorbidities, this difference can be clinically meaningful, reinforcing the preference for injectable therapies in high-risk patient populations.
Safety and tolerability also remain key considerations. Oral GLP-1 therapies are frequently associated with gastrointestinal side effects, including nausea, diarrhea, constipation, and vomiting. Although these adverse events are generally similar to those seen with injectable formulations, they can become more prominent during dose escalation and titration periods. Recent clinical studies have shown improved tolerability compared with earlier danuglipron data; however, treatment discontinuation and patient adherence are still expected to remain important real-world challenges.
Insurance coverage represents another major barrier to broader adoption. Reimbursement for obesity-focused GLP-1 therapies remains inconsistent, particularly for oral formulations indicated for obesity management. At present, only about 55% of commercial employers provide coverage for GLP-1 obesity therapies, while nearly 15% have already reduced or eliminated coverage because of escalating treatment costs. Although oral therapies may eventually improve pricing flexibility and patient accessibility, they are unlikely to fully address payer concerns regarding affordability and long-term reimbursement sustainability.
Manufacturing capacity and supply scalability pose additional risks, especially during the early stages of commercialization. Both Novo Nordisk and Eli Lilly have invested heavily in expanding manufacturing infrastructure for oral GLP-1 therapies, including facilities across North Carolina, Texas, Alabama, and Puerto Rico. Nevertheless, despite these substantial investments, supply limitations and production bottlenecks may still arise as global demand continues to increase rapidly following product launches.
Importantly, injectable therapies such as WEGOVY and ZEPBOUND are unlikely to lose relevance. Their superior weight-loss efficacy ensures they will continue to serve as the clinical benchmark for patients requiring maximum therapeutic benefit and who are comfortable with injectable administration. The future obesity treatment landscape will likely evolve into a more personalized and tiered approach, with oral therapies supporting treatment initiation, maintenance, and convenience-focused use cases; high-efficacy injectable therapies reserved for intensive intervention; and next-generation triple agonists and combination regimens targeting more complex patient populations.
What remains clear is that the obesity therapeutics market, already among the fastest-growing segments in pharmaceutical history, is entering a dramatically larger phase of expansion. The arrival of oral GLP-1 therapies marks the beginning of a new chapter in obesity pharmacotherapy.

Downloads
Article in PDF
Recent Articles
- Redefining Liver Disease in the Metabolic Era: From NASH to MASH and the Rise of Obesity‐targeted...
- Hengrui Pharma Encounters FDA Regulatory Hurdle for Camrelizumab–Rivoceranib; Kailera Therapeutic...
- Lilly’s ZEPBOUND Clears Hurdle in Sleep Apnea Treatment
- 8 Emerging Obesity Trends Transforming Therapeutics Segment
- 9 Promising Obesity Drugs Set to Launch by 2030



