HomeBlog Alzheimers disease treatment and clinical trials
Challenges in the Pursuit of Alzheimer’s Disease Treatment Breakthroughs: Drug Clinical Trial Failures
Feb 12, 2025
Alzheimer’s, the most common type of dementia, particularly with an increasing geriatric population, presents a major global crisis. The disease mostly occurs in sexagenarians, but it may manifest in quadragenarians. It is one of the most prevalent neurodegenerative disorders with a multifactorial pathogenesis. It is characterized by a gradual decline in cognitive and functional abilities, with individuals eventually losing their capability to undertake everyday tasks and function independently. Alzheimer’s disease is one of the top ten leading causes of death in the US and the fifth leading cause of death among adults aged 65 years or older.
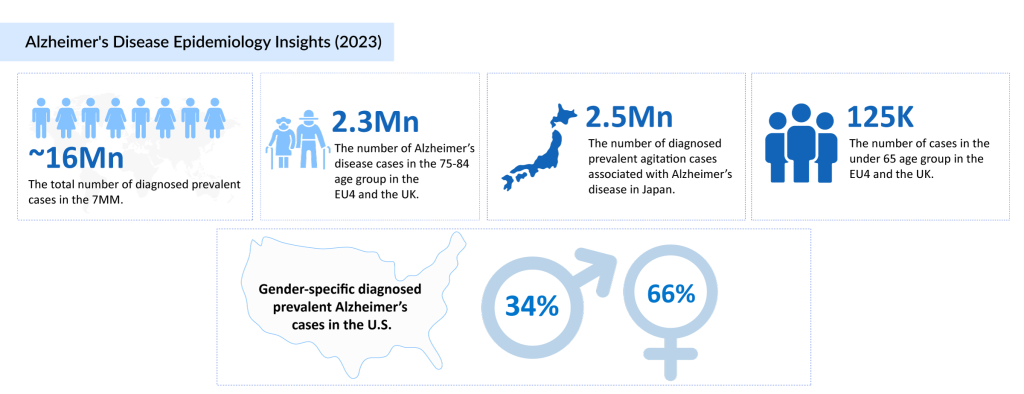
“According to DelveInsight’s epidemiology analysis, the age cohort 75─84 years accounted for the highest, nearly 44% (approximately 7 million) of the total diagnosed prevalent cases of Alzheimer’s disease in the 7MM.”
It is widely known that the progressive cognitive decline as a result of Alzheimer’s disease is associated with the accumulation of amyloid-beta and tau proteins, leading to the formation of two underlying pathological hallmarks, extracellular amyloid beta plaques and intracellular neurofibrillary tangles. These disrupt communication between brain cells, leading to their degeneration.
However, advancements in the comprehensive understanding of disease pathophysiology and the discovery of novel signaling pathways have revolutionized disease diagnosis, making it more personalized, timely, and reliable. Initiating early treatment is a basic tenant to slow disease progression.
The current Alzheimer’s disease treatment regime is not curative and mostly includes symptomatic therapies. The Alzheimer’s disease treatment market has made considerable progress, with new developments, especially in the past five years, with more amyloid beta-proteins targeted monoclonal antibodies entering the Alzheimer’s disease treatment market, besides the more common acetylcholinesterase inhibitors (AChEIs) and NMDA receptor antagonists.
The recent approval of monoclonal antibodies is a glimmer of hope in the Alzheimer’s disease emerging drug landscape littered with failures in recent years. In the chase to enter the lucrative Alzheimer’s market, many drugs that were deemed game changers have failed in late stages. Recent failures include phase III studies across targets such as γ-secretase inhibitors, β secretase inhibitors, monoclonal antibodies, and intravenous immunoglobulins in patients with early-stage, mild, or mild to moderate Alzheimer’s. Additionally, some tau aggregation inhibitors have also failed in the late stage.
The list of failures is long, but the crucial ones to drop out of the race from 2023 to 2024 include Eli Lilly’s LY3372689, Athira Pharma’s Fosgonimeton, Sage Therapeutics’ Dalzanemdor, Avanir Pharmaceuticals’ Deudextromethorphan, Roche/Chugai’s gantenerumab, Merck’s verubecestat, Eli Lilly’s solanezumab, AstraZeneca and Eli Lilly’s lanabecestat, Novartis and Amgen’s CNP520 (umibecestat), Johnson & Johnson’s atabecestat, among others.
Inhibitors of γ-Secretase abandoned in phase III studies included semagecestat avagacestat and tarenflurbil. Semagecestat was associated with worsening of daily function and increased rates of skin cancer and infection. In contrast, avagacestat was associated with a higher progression rate of the disease and adverse dose-limiting effects like skin cancer, and tarenflurbil was ascribed to low potency and brain penetration.
The past decade has appeared optimistic for finding disease-modifying therapies for Alzheimer’s as a result of the understanding of the “amyloid hypothesis”, especially with several BACE inhibitors in clinical trials. However, what happened could be described as a burial ground for BACE inhibitors, with almost all pharmaceutical companies having abandoned BACE1 inhibitors. No BACE inhibitor is listed in any company’s pipeline for experimental or clinical development.
BACE1 inhibitor, lanabecestat, a collaborative therapy of AstraZeneca and Eli Lilly, having skipped Phase II trials and directly begun Phase III, was discontinued in 2018. The trials were put to end for futility, as they were not likely to meet the primary endpoints upon completion. Janssen’s atabecestat, despite a long history of clinical trials with promising results, was unable to progress beyond phase II/III study, due to reports of liver toxicity in test subjects. The drug was discontinued in 2018.
Merck’s verubecestat and Biogen and Eisai’s elenbecestat, also BACE1 inhibitors, were dropped from the pipeline, as Phase III results demonstrated no benefits in mitigating cognitive/functional decline in patients with Alzheimer’s. Rather, they had unfavorable risk-benefit ratios associated with cognitive worsening, brain volume loss, and multiple treatment-related adverse events, including falls and injuries, suicidal ideation, weight loss, sleep disturbance, skin rash, and hair color change.
Novartis and Amgen’s umibecestat was discontinued due to reports of safety issues, and Eli Lilly’s LY3202626 abandoned due to the low likelihood of statistically significant treatment effect.
A multitude of trials were underway for other mechanisms of action, like amyloid-beta-specific monoclonal antibodies, tau-aggregate inhibitors, and tau vaccines, among others. Amyloid-beta targeting drugs were touted as game-changers, however many of these also failed in gaining market entry, casting doubt on the validity of amyloid as a target – until recently.
Eli Lilly, solanezumab, an Aβ-specific mAb, designed to target soluble forms of amyloid beta, did not clear existing plaques and was abandoned by Lilly in 2016 after it did not slow loss of mental functioning in patients with mild Alzheimer’s symptoms in clinical trials.
Roche’s Genentech and AC Immune’s drug, crenezumab, failed to prevent early symptoms or slow cognitive decline. There was no significant difference in cognition or the ability to store and retrieve new memories between participants who received the drug and those who got a placebo. After a decade of efforts, the company bid adieu to the drug in 2022.
Another big blow was Roche (Genentech’s) gantenerumab, as the drug missed the mark, and was unable to slow clinical decline in people with early-stage disease but also did not seem to clear amyloid plaques.
In August 2024, Eli Lilly, a major player in Alzheimer’s drug development, faced a significant setback. Their experimental anti-tau drug LY3372689, designed to prevent the buildup of tau tangles—one of the disease’s hallmarks—failed in its Phase 2 clinical trial. The trial, which aimed to test whether the drug could slow cognitive decline in early symptomatic Alzheimer’s patients, did not meet its primary endpoint. The disappointment was palpable. Tau pathology has long been considered a critical target in AD, and Lilly had hoped that LY3372689 would be the next big step following the approval of their anti-amyloid drug, Kisunla (donanemab). But when the data came in, it showed that patients on the drug did no better than those on a placebo. While Lilly remains committed to exploring tau-targeting therapies, this failure left them without a single tau-directed candidate in their clinical-stage pipeline.
Just a month later, inSeptember 2024, Athira Pharma experienced disappointment when fosgonimeton, an investigational treatment, failed to demonstrate significant cognitive improvements in a Phase 2/3 clinical trial. Fosgonimeton was designed to enhance brain function by targeting neurotrophic pathways. Still, despite being well tolerated, the drug did not lead to meaningful improvements in cognitive skills or daily functioning in patients with mild to moderate Alzheimer’s. Researchers pointed to potential flaws in the trial, such as the relatively short 26-week treatment period and the fact that the placebo group showed little cognitive decline—making it difficult to measure any real benefit. Though the drug showed some minor advantages in select subgroups, such as those carrying the APOE4 gene, the results were not strong enough to justify moving forward.
Then came another blow inOctober 2024, when Sage Therapeutics announced that it was halting the development of dalzanemdor (SAGE-718) for Alzheimer’s disease. The LIGHTWAVE study, which tested the drug in patients with mild cognitive impairment and early-stage dementia, failed to show any meaningful improvement in cognitive function. Sage had pinned its hopes on dalzanemdor’s ability to enhance NMDA receptor activity, a key player in neural communication and memory formation. However, despite the drug’s promising mechanism of action and favorable safety profile, it ultimately fell short in clinical trials. In the wake of this failure, Sage made the difficult decision to discontinue further research into dalzanemdor for AD, shifting its focus to other neuropsychiatric conditions.
Even before these recent setbacks, inFebruary 2024, Otsuka Pharmaceutical faced its own challenges when its Phase 3 trial of AVP-786 failed to meet its main goal of easing agitation in Alzheimer’s patients. The drug was being evaluated as a potential treatment for agitation associated with dementia, a symptom that can be distressing for both patients and caregivers. Unfortunately, the trial results showed no significant difference between the drug and placebo, and to make matters worse, there was a higher rate of falls among patients receiving AVP-786. While Otsuka has vowed to analyze the data further to see if the drug might still have potential, this failure has cast doubt on AVP-786’s future as an Alzheimer’s treatment.
These repeated disappointments serve as a stark reminder of how complex and elusive Alzheimer’s disease remains. Researchers continue to pursue different therapeutic targets—beta-amyloid plaques, tau tangles, neuroinflammation, and metabolic dysfunction—but the road to an effective treatment is long and unpredictable. For every breakthrough like Leqembi (lecanemab) and Kisunla (donanemab), multiple failed drugs never make it past clinical trials. Yet, despite these setbacks, the scientific community remains undeterred. The lessons learned from these failures will help refine future research, bringing us one step closer to an effective therapy—or even a cure—for Alzheimer’s disease.
Most of these failures can be attributed to:
Inadequate understanding of the complex pathophysiology of Alzheimer’s disease that has led to the incorrect selection of treatment targets and inappropriate drug dosages
Insufficient evidence for initiating pivotal trials and testing for clinical efficacy, as drugs advanced into the pivotal phase III trial for Alzheimer’s disease with far less efficacy testing than generally accepted in standard practice
Studies relied on and accepted changes in biomarker levels (Aβ or tau) as surrogate clinical endpoints without evidence of confirmatory changes in cognitive, functional, and global performance when deciding to advance to the pivotal trial.
Pivotal trial design issues such as poor choice of primary clinical outcome measures, inclusion of non-Alzheimer patients, insufficient accounting for Alzheimer’s subtype, and late intervention administration further added to the troubles.
Despite high failure rates, companies are holding on to hope and tirelessly seeking the key to unlock effective treatments and renewed possibilities for Alzheimer’s disease to change the treatment paradigm in the years to come.
“Every step we take towards better Alzheimer’s disease treatment is a step closer to a brighter tomorrow for millions of families touched by this disease.”
The US FDA’s accelerated approval of Biogen and Eisai‘s ADUHELM is a glimmer of hope amidst the successive chain of failures. Though the approval was not without controversy, given that the data it was based on was less than solid, the decision left the door ajar for further approvals based on surrogate biomarker data.
The FDA conversion of Biogen and Eisai’s LEQEMBI’s (lecanemab) accelerated approval to a traditional one, which is a classic example of grit and persistence. Despite a few initial hiccups, the approval, along with a CMS go-ahead with Medicare covering the therapy for Alzheimer’s appropriate patient segment, has provided much relief. Besides garnering support for Biogen and Eisai and helping them drive past the ADUHELM stumble, this approval has opened the gates for a plethora of therapies in different stages of development.
Late-stage trial results of Eli Lilly’s donanemab, wherein it slows cognitive decline by 35%, is another unexpected success and is hailed as a ‘turning point’ for Alzheimer’s disease treatment. Both these provide strong evidence that removing amyloid from the brain can slow down Alzheimer’s disease, and the amyloid hypothesis, whose potential had been uncertain after dozens of drug failures, actually has disease-modifying potential.
Transforming the Alzheimer’s Treatment Landscape: A New Era of Innovation
The fight against Alzheimer’s disease is witnessing a remarkable shift, with groundbreaking advancements redefining the treatment and diagnosis of this devastating condition. In just the first few weeks of 2025, a series of critical regulatory milestones and scientific breakthroughs have signaled that hope is on the horizon for millions affected by the disease.
At the forefront of these developments is Spear Bio Inc.’s pTau 217 blood test, which recently received Breakthrough Device Designation from the FDA. This test has the potential to revolutionize early detection by providing a simple yet highly sensitive diagnostic tool, helping to identify Alzheimer’s disease long before symptoms progress. Early detection has long been a missing piece in the Alzheimer’s treatment puzzle, and Spear Bio’s test could bridge that gap, ensuring patients receive timely interventions.
Meanwhile, the treatment landscape is also rapidly evolving. BioArctic AB and Eisai are pushing the boundaries of convenience in Alzheimer’s therapy, with the FDA accepting the Biologics License Application (BLA) for the Leqembi subcutaneous autoinjector (SC-AI). This weekly maintenance dosing option could make treatment significantly more accessible, reducing the need for complex intravenous infusions and enabling patients to manage their condition more effectively at home.
In parallel, the Fast Track designation for posdinemab, a monoclonal antibody targeting phosphorylated tau, marks another crucial step in addressing the underlying pathology of Alzheimer’s disease. Being evaluated in the phase 2b AuTonomy study, posdinemab represents a novel approach aimed at slowing disease progression by tackling one of the key hallmarks of Alzheimer’s—tau protein accumulation.
Adding to the momentum, Axsome Therapeutics is preparing to seek FDA approval for AXS-05 in Alzheimer’s-related agitation, despite mixed results in clinical trials. AXS-05, a combination of dextromethorphan and bupropion, has already shown promise in major depressive disorder, and if approved, could offer a much-needed solution for managing behavioral symptoms associated with Alzheimer’s, improving both patient well-being and caregiver burden.
The advancements are not limited to the U.S. market. In December 2024, Eli Lilly achieved a major milestone with the approval of Kisunla in China. As the world’s second-largest pharmaceutical market, China’s regulatory green light for this anti-amyloid therapy signifies a growing global commitment to tackling Alzheimer’s disease and expanding access to innovative treatments.
Beyond drug development, quantitative systems pharmacology (QSP) models combined with artificial intelligence (AI) are playing an increasing role in Alzheimer’s research. These advanced modeling techniques help identify gaps in our knowledge, generate new biological or pharmacological hypotheses, and guide the design of in vitro and in vivo experiments. Scientists have already begun applying AI-driven modeling to Alzheimer’s with promising results—AI models have demonstrated high accuracy in diagnosing Alzheimer’s patients, further supporting early detection efforts and personalized treatment approaches.
Together, these breakthroughs highlight a dynamic shift in the Alzheimer’s landscape, from improved diagnostics to more accessible treatments and novel therapeutic approaches. With continued innovation, AI integration, and regulatory support, 2025 could mark the beginning of a new era in Alzheimer’s care—one that prioritizes early detection, patient-friendly treatment options, and disease-modifying therapies that could ultimately change the course of this condition.
Various therapies by AB Science, Alzheon Inc., AriBio Co., Ltd., AgeneBio, Inc., Anavex Life Sciences Corp., Annovis Bio, Inc., Cerecin, BioVie, Cassava Sciences, Novo Nordisk, Eli Lilly, Neurim Pharmaceuticals, Suven Life Sciences, Bristol Myers Squibb/Karuna Therapeutics, T3D Therapeutics, Inc., Lexeo Therapeutics, Axsome Therapeutics, Inc., Araclon Biotech S.L., Eisai Co., Ltd., TauRx Therapeutics, TrueBinding, Inc., AC Immune SA/Johnson & Johnson, Longeveron Inc., Vaccinex Inc., IGC Pharma LLC., others are in late stages of development that have the potential to create a positive shift in the Alzheimer’s disease treatment market.
The early-stage Alzheimer’s disease pipeline is complete with therapies with novel mechanisms of action, and improved disease pathology has added to this growth of drug development. The early Alzheimer’s pipeline is brimming with biggies like Janssen, AbbVie, Merck, etc., which are also in the race. With several assets being assessed, what is certain is that even though a few might fail, there will be improved treatment, and the Alzheimer’s disease treatment market will grow leaps and bounds in the future.
Therefore, despite the present challenges, there is a positive force in improving Alzheimer’s disease treatment. With innovative drug development, the path toward a world where memory endures, cognition thrives, and the specter of Alzheimer’s disease is but a distant memory looks optimistic.
Challenges in the Pursuit of Alzheimer’s Disease Treatment Breakthroughs: Drug Clinical Trial Failures
Feb 12, 2025
Alzheimer’s, the most common type of dementia, particularly with an increasing geriatric population, presents a major global crisis. The disease mostly occurs in sexagenarians, but it may manifest in quadragenarians. It is one of the most prevalent neurodegenerative disorders with a multifactorial pathogenesis. It is characterized by a gradual decline in cognitive and functional abilities, with individuals eventually losing their capability to undertake everyday tasks and function independently. Alzheimer’s disease is one of the top ten leading causes of death in the US and the fifth leading cause of death among adults aged 65 years or older.
“According to DelveInsight’s epidemiology analysis, the age cohort 75─84 years accounted for the highest, nearly 44% (approximately 7 million) of the total diagnosed prevalent cases of Alzheimer’s disease in the 7MM.”
It is widely known that the progressive cognitive decline as a result of Alzheimer’s disease is associated with the accumulation of amyloid-beta and tau proteins, leading to the formation of two underlying pathological hallmarks, extracellular amyloid beta plaques and intracellular neurofibrillary tangles. These disrupt communication between brain cells, leading to their degeneration.
However, advancements in the comprehensive understanding of disease pathophysiology and the discovery of novel signaling pathways have revolutionized disease diagnosis, making it more personalized, timely, and reliable. Initiating early treatment is a basic tenant to slow disease progression.
The current Alzheimer’s disease treatment regime is not curative and mostly includes symptomatic therapies. The Alzheimer’s disease treatment market has made considerable progress, with new developments, especially in the past five years, with more amyloid beta-proteins targeted monoclonal antibodies entering the Alzheimer’s disease treatment market, besides the more common acetylcholinesterase inhibitors (AChEIs) and NMDA receptor antagonists.
The recent approval of monoclonal antibodies is a glimmer of hope in the Alzheimer’s disease emerging drug landscape littered with failures in recent years. In the chase to enter the lucrative Alzheimer’s market, many drugs that were deemed game changers have failed in late stages. Recent failures include phase III studies across targets such as γ-secretase inhibitors, β secretase inhibitors, monoclonal antibodies, and intravenous immunoglobulins in patients with early-stage, mild, or mild to moderate Alzheimer’s. Additionally, some tau aggregation inhibitors have also failed in the late stage.
The list of failures is long, but the crucial ones to drop out of the race from 2023 to 2024 include Eli Lilly’s LY3372689, Athira Pharma’s Fosgonimeton, Sage Therapeutics’ Dalzanemdor, Avanir Pharmaceuticals’ Deudextromethorphan, Roche/Chugai’s gantenerumab, Merck’s verubecestat, Eli Lilly’s solanezumab, AstraZeneca and Eli Lilly’s lanabecestat, Novartis and Amgen’s CNP520 (umibecestat), Johnson & Johnson’s atabecestat, among others.
Inhibitors of γ-Secretase abandoned in phase III studies included semagecestat avagacestat and tarenflurbil. Semagecestat was associated with worsening of daily function and increased rates of skin cancer and infection. In contrast, avagacestat was associated with a higher progression rate of the disease and adverse dose-limiting effects like skin cancer, and tarenflurbil was ascribed to low potency and brain penetration.
The past decade has appeared optimistic for finding disease-modifying therapies for Alzheimer’s as a result of the understanding of the “amyloid hypothesis”, especially with several BACE inhibitors in clinical trials. However, what happened could be described as a burial ground for BACE inhibitors, with almost all pharmaceutical companies having abandoned BACE1 inhibitors. No BACE inhibitor is listed in any company’s pipeline for experimental or clinical development.
BACE1 inhibitor, lanabecestat, a collaborative therapy of AstraZeneca and Eli Lilly, having skipped Phase II trials and directly begun Phase III, was discontinued in 2018. The trials were put to end for futility, as they were not likely to meet the primary endpoints upon completion. Janssen’s atabecestat, despite a long history of clinical trials with promising results, was unable to progress beyond phase II/III study, due to reports of liver toxicity in test subjects. The drug was discontinued in 2018.
Merck’s verubecestat and Biogen and Eisai’s elenbecestat, also BACE1 inhibitors, were dropped from the pipeline, as Phase III results demonstrated no benefits in mitigating cognitive/functional decline in patients with Alzheimer’s. Rather, they had unfavorable risk-benefit ratios associated with cognitive worsening, brain volume loss, and multiple treatment-related adverse events, including falls and injuries, suicidal ideation, weight loss, sleep disturbance, skin rash, and hair color change.
Novartis and Amgen’s umibecestat was discontinued due to reports of safety issues, and Eli Lilly’s LY3202626 abandoned due to the low likelihood of statistically significant treatment effect.
A multitude of trials were underway for other mechanisms of action, like amyloid-beta-specific monoclonal antibodies, tau-aggregate inhibitors, and tau vaccines, among others. Amyloid-beta targeting drugs were touted as game-changers, however many of these also failed in gaining market entry, casting doubt on the validity of amyloid as a target – until recently.
Eli Lilly, solanezumab, an Aβ-specific mAb, designed to target soluble forms of amyloid beta, did not clear existing plaques and was abandoned by Lilly in 2016 after it did not slow loss of mental functioning in patients with mild Alzheimer’s symptoms in clinical trials.
Roche’s Genentech and AC Immune’s drug, crenezumab, failed to prevent early symptoms or slow cognitive decline. There was no significant difference in cognition or the ability to store and retrieve new memories between participants who received the drug and those who got a placebo. After a decade of efforts, the company bid adieu to the drug in 2022.
Another big blow was Roche (Genentech’s) gantenerumab, as the drug missed the mark, and was unable to slow clinical decline in people with early-stage disease but also did not seem to clear amyloid plaques.
In August 2024, Eli Lilly, a major player in Alzheimer’s drug development, faced a significant setback. Their experimental anti-tau drug LY3372689, designed to prevent the buildup of tau tangles—one of the disease’s hallmarks—failed in its Phase 2 clinical trial. The trial, which aimed to test whether the drug could slow cognitive decline in early symptomatic Alzheimer’s patients, did not meet its primary endpoint. The disappointment was palpable. Tau pathology has long been considered a critical target in AD, and Lilly had hoped that LY3372689 would be the next big step following the approval of their anti-amyloid drug, Kisunla (donanemab). But when the data came in, it showed that patients on the drug did no better than those on a placebo. While Lilly remains committed to exploring tau-targeting therapies, this failure left them without a single tau-directed candidate in their clinical-stage pipeline.
Just a month later, inSeptember 2024, Athira Pharma experienced disappointment when fosgonimeton, an investigational treatment, failed to demonstrate significant cognitive improvements in a Phase 2/3 clinical trial. Fosgonimeton was designed to enhance brain function by targeting neurotrophic pathways. Still, despite being well tolerated, the drug did not lead to meaningful improvements in cognitive skills or daily functioning in patients with mild to moderate Alzheimer’s. Researchers pointed to potential flaws in the trial, such as the relatively short 26-week treatment period and the fact that the placebo group showed little cognitive decline—making it difficult to measure any real benefit. Though the drug showed some minor advantages in select subgroups, such as those carrying the APOE4 gene, the results were not strong enough to justify moving forward.
Then came another blow inOctober 2024, when Sage Therapeutics announced that it was halting the development of dalzanemdor (SAGE-718) for Alzheimer’s disease. The LIGHTWAVE study, which tested the drug in patients with mild cognitive impairment and early-stage dementia, failed to show any meaningful improvement in cognitive function. Sage had pinned its hopes on dalzanemdor’s ability to enhance NMDA receptor activity, a key player in neural communication and memory formation. However, despite the drug’s promising mechanism of action and favorable safety profile, it ultimately fell short in clinical trials. In the wake of this failure, Sage made the difficult decision to discontinue further research into dalzanemdor for AD, shifting its focus to other neuropsychiatric conditions.
Even before these recent setbacks, inFebruary 2024, Otsuka Pharmaceutical faced its own challenges when its Phase 3 trial of AVP-786 failed to meet its main goal of easing agitation in Alzheimer’s patients. The drug was being evaluated as a potential treatment for agitation associated with dementia, a symptom that can be distressing for both patients and caregivers. Unfortunately, the trial results showed no significant difference between the drug and placebo, and to make matters worse, there was a higher rate of falls among patients receiving AVP-786. While Otsuka has vowed to analyze the data further to see if the drug might still have potential, this failure has cast doubt on AVP-786’s future as an Alzheimer’s treatment.
These repeated disappointments serve as a stark reminder of how complex and elusive Alzheimer’s disease remains. Researchers continue to pursue different therapeutic targets—beta-amyloid plaques, tau tangles, neuroinflammation, and metabolic dysfunction—but the road to an effective treatment is long and unpredictable. For every breakthrough like Leqembi (lecanemab) and Kisunla (donanemab), multiple failed drugs never make it past clinical trials. Yet, despite these setbacks, the scientific community remains undeterred. The lessons learned from these failures will help refine future research, bringing us one step closer to an effective therapy—or even a cure—for Alzheimer’s disease.
Most of these failures can be attributed to:
Inadequate understanding of the complex pathophysiology of Alzheimer’s disease that has led to the incorrect selection of treatment targets and inappropriate drug dosages
Insufficient evidence for initiating pivotal trials and testing for clinical efficacy, as drugs advanced into the pivotal phase III trial for Alzheimer’s disease with far less efficacy testing than generally accepted in standard practice
Studies relied on and accepted changes in biomarker levels (Aβ or tau) as surrogate clinical endpoints without evidence of confirmatory changes in cognitive, functional, and global performance when deciding to advance to the pivotal trial.
Pivotal trial design issues such as poor choice of primary clinical outcome measures, inclusion of non-Alzheimer patients, insufficient accounting for Alzheimer’s subtype, and late intervention administration further added to the troubles.
Despite high failure rates, companies are holding on to hope and tirelessly seeking the key to unlock effective treatments and renewed possibilities for Alzheimer’s disease to change the treatment paradigm in the years to come.
“Every step we take towards better Alzheimer’s disease treatment is a step closer to a brighter tomorrow for millions of families touched by this disease.”
The US FDA’s accelerated approval of Biogen and Eisai‘s ADUHELM is a glimmer of hope amidst the successive chain of failures. Though the approval was not without controversy, given that the data it was based on was less than solid, the decision left the door ajar for further approvals based on surrogate biomarker data.
The FDA conversion of Biogen and Eisai’s LEQEMBI’s (lecanemab) accelerated approval to a traditional one, which is a classic example of grit and persistence. Despite a few initial hiccups, the approval, along with a CMS go-ahead with Medicare covering the therapy for Alzheimer’s appropriate patient segment, has provided much relief. Besides garnering support for Biogen and Eisai and helping them drive past the ADUHELM stumble, this approval has opened the gates for a plethora of therapies in different stages of development.
Late-stage trial results of Eli Lilly’s donanemab, wherein it slows cognitive decline by 35%, is another unexpected success and is hailed as a ‘turning point’ for Alzheimer’s disease treatment. Both these provide strong evidence that removing amyloid from the brain can slow down Alzheimer’s disease, and the amyloid hypothesis, whose potential had been uncertain after dozens of drug failures, actually has disease-modifying potential.
Transforming the Alzheimer’s Treatment Landscape: A New Era of Innovation
The fight against Alzheimer’s disease is witnessing a remarkable shift, with groundbreaking advancements redefining the treatment and diagnosis of this devastating condition. In just the first few weeks of 2025, a series of critical regulatory milestones and scientific breakthroughs have signaled that hope is on the horizon for millions affected by the disease.
At the forefront of these developments is Spear Bio Inc.’s pTau 217 blood test, which recently received Breakthrough Device Designation from the FDA. This test has the potential to revolutionize early detection by providing a simple yet highly sensitive diagnostic tool, helping to identify Alzheimer’s disease long before symptoms progress. Early detection has long been a missing piece in the Alzheimer’s treatment puzzle, and Spear Bio’s test could bridge that gap, ensuring patients receive timely interventions.
Meanwhile, the treatment landscape is also rapidly evolving. BioArctic AB and Eisai are pushing the boundaries of convenience in Alzheimer’s therapy, with the FDA accepting the Biologics License Application (BLA) for the Leqembi subcutaneous autoinjector (SC-AI). This weekly maintenance dosing option could make treatment significantly more accessible, reducing the need for complex intravenous infusions and enabling patients to manage their condition more effectively at home.
In parallel, the Fast Track designation for posdinemab, a monoclonal antibody targeting phosphorylated tau, marks another crucial step in addressing the underlying pathology of Alzheimer’s disease. Being evaluated in the phase 2b AuTonomy study, posdinemab represents a novel approach aimed at slowing disease progression by tackling one of the key hallmarks of Alzheimer’s—tau protein accumulation.
Adding to the momentum, Axsome Therapeutics is preparing to seek FDA approval for AXS-05 in Alzheimer’s-related agitation, despite mixed results in clinical trials. AXS-05, a combination of dextromethorphan and bupropion, has already shown promise in major depressive disorder, and if approved, could offer a much-needed solution for managing behavioral symptoms associated with Alzheimer’s, improving both patient well-being and caregiver burden.
The advancements are not limited to the U.S. market. In December 2024, Eli Lilly achieved a major milestone with the approval of Kisunla in China. As the world’s second-largest pharmaceutical market, China’s regulatory green light for this anti-amyloid therapy signifies a growing global commitment to tackling Alzheimer’s disease and expanding access to innovative treatments.
Beyond drug development, quantitative systems pharmacology (QSP) models combined with artificial intelligence (AI) are playing an increasing role in Alzheimer’s research. These advanced modeling techniques help identify gaps in our knowledge, generate new biological or pharmacological hypotheses, and guide the design of in vitro and in vivo experiments. Scientists have already begun applying AI-driven modeling to Alzheimer’s with promising results—AI models have demonstrated high accuracy in diagnosing Alzheimer’s patients, further supporting early detection efforts and personalized treatment approaches.
Together, these breakthroughs highlight a dynamic shift in the Alzheimer’s landscape, from improved diagnostics to more accessible treatments and novel therapeutic approaches. With continued innovation, AI integration, and regulatory support, 2025 could mark the beginning of a new era in Alzheimer’s care—one that prioritizes early detection, patient-friendly treatment options, and disease-modifying therapies that could ultimately change the course of this condition.
Various therapies by AB Science, Alzheon Inc., AriBio Co., Ltd., AgeneBio, Inc., Anavex Life Sciences Corp., Annovis Bio, Inc., Cerecin, BioVie, Cassava Sciences, Novo Nordisk, Eli Lilly, Neurim Pharmaceuticals, Suven Life Sciences, Bristol Myers Squibb/Karuna Therapeutics, T3D Therapeutics, Inc., Lexeo Therapeutics, Axsome Therapeutics, Inc., Araclon Biotech S.L., Eisai Co., Ltd., TauRx Therapeutics, TrueBinding, Inc., AC Immune SA/Johnson & Johnson, Longeveron Inc., Vaccinex Inc., IGC Pharma LLC., others are in late stages of development that have the potential to create a positive shift in the Alzheimer’s disease treatment market.
The early-stage Alzheimer’s disease pipeline is complete with therapies with novel mechanisms of action, and improved disease pathology has added to this growth of drug development. The early Alzheimer’s pipeline is brimming with biggies like Janssen, AbbVie, Merck, etc., which are also in the race. With several assets being assessed, what is certain is that even though a few might fail, there will be improved treatment, and the Alzheimer’s disease treatment market will grow leaps and bounds in the future.
Therefore, despite the present challenges, there is a positive force in improving Alzheimer’s disease treatment. With innovative drug development, the path toward a world where memory endures, cognition thrives, and the specter of Alzheimer’s disease is but a distant memory looks optimistic.