Drug-Resistant Epilepsy: Evolving Treatment Strategies for a High‑Unmet‑Need Population
Feb 09, 2026
Table of Contents
Summary
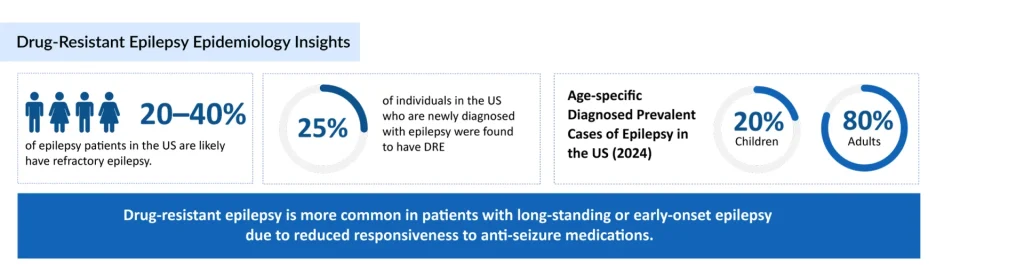
- Drug-resistant epilepsy affects 20-40% of epilepsy patients in the US, rising to 30-40% in adults versus 7-20% in children, with similar rates (over 25%) in Europe; about one-quarter of newly diagnosed cases progress to DRE.
- Vagus Nerve Stimulation (VNS Therapy by LivaNova) is FDA-approved for drug-resistant partial/generalized seizures (including pediatrics ≥4 years since 2017); LivaNova sought broader Medicare coverage in June 2025.
- Some of the therapies and devices in the pipeline include NRTX-1001 [Neurona Therapeutics ((NMRA)], IAMA-6 (IAMA Therapeutics), BM-101 [(Bright Minds Bio ((NASDAQ: DRUG)], and others.
Epilepsy affects millions of people worldwide, and for most, anti‑seizure medications (ASMs) are effective in achieving good seizure control. However, for a substantial subset of patients, seizures persist despite appropriate medical therapy. This condition, known as drug‑resistant epilepsy (DRE) or refractory epilepsy, remains one of the most challenging areas in neurology and a major driver of unmet clinical and commercial need.
Downloads
Click Here To Get the Article in PDF

Recent Articles
- EPIDIOLEX and FINTEPLA in 2026: Commercial Anchors in a Precision DEE Pipeline
- Can Cannabinoids be an Effective Medicinal Substance?
- DRUG-RESISTANT EPILEPSY
- Role of Seizures Alert and Monitoring Devices in the Management of Epilepsy
- CAR-T in killing tumors; Amunix raises $73M; Autism findings in protein-targeted treatment
DRE is typically defined as the failure of adequate trials of two tolerated, appropriately chosen, and used ASMs (alone or in combination) to achieve sustained seizure freedom. Once a patient meets this definition, the likelihood that adding or switching to additional medications will fully control seizures declines substantially, and the focus shifts to advanced interventions and emerging therapies.
The Burden of Drug-Resistant Epilepsy
Epidemiological analyses across major markets suggest that around 20–40% of people living with epilepsy in the US may have refractory disease, and DRE is more common in adults than in children. While approximately 7–20% of children with epilepsy struggle to control their seizures with available medications, this proportion climbs to 30–40% in adults. Real‑world data from Europe similarly highlight a high and persistent disease burden, with about one‑quarter of newly diagnosed epilepsy patients in the US eventually meeting criteria for DRE, and recent UK estimates indicating DRE prevalence of more than one in four epilepsy patients.
This burden goes far beyond seizure counts. Uncontrolled epilepsy is linked to injuries, cognitive and psychiatric comorbidities, social isolation, loss of independence, and increased mortality risk. Healthcare utilization is also disproportionately high in this group, with recurrent emergency visits, hospitalizations, and long‑term disability.
Current Drug-Resistant Epilepsy Treatment Approaches
Management of DRE is inherently multidisciplinary. Once a patient is identified as drug‑resistant, referral to a specialized epilepsy center is strongly recommended to reassess the diagnosis, optimize therapy, and evaluate advanced treatment options.
Optimizing Pharmacotherapy
Pharmacologic therapy remains the foundation of epilepsy care, even in the drug‑resistant setting. Many individuals with DRE are on multiple ASMs, often at high doses, aiming to reduce seizure frequency and severity. Key drug classes include:
- Sodium channel modulators (e.g., phenytoin, carbamazepine, oxcarbazepine, lamotrigine) that stabilize neuronal membranes and limit repetitive firing.
- GABAergic modulators that enhance inhibitory neurotransmission.
- Calcium channel blockers, synaptic vesicle (SV2A) modulators, and receptor antagonists are used alone or in rational polytherapy.
Phenytoin and carbamazepine are long‑standing agents that primarily act via voltage‑gated sodium channel blockade. Oxcarbazepine exerts similar antiepileptic activity but tends to be better tolerated with fewer drug–drug interactions. Newer agents such as cenobamate, perampanel, cannabidiol, and ganaxolone are increasingly used in refractory disease, even though they are labeled for specific seizure types or syndromes rather than DRE as a distinct indication.
Despite these epilepsy treatment options, evidence shows that once two adequately chosen, tolerated ASMs have failed, the probability of achieving complete seizure freedom with further drug changes or combinations is relatively low. At that point, additional strategies become critical.
Epilepsy Surgery
For focal epilepsies, especially temporal lobe epilepsy, resective brain surgery can offer the highest chance of long‑term seizure freedom. Surgical options include:
- Temporal lobectomy or lesionectomy for patients with well‑defined seizure foci
- Disconnection procedures in appropriately selected cases
Surgical candidacy depends on the precise localization of the epileptogenic zone, assessment of cognitive and functional risk, and multidisciplinary evaluation. When feasible and safe, surgery can transform quality of life, but many patients are not suitable candidates or are reluctant to undergo invasive brain procedures.
Neuromodulation Therapies
For individuals who are not candidates for resective surgery or who continue to have seizures after surgery, neuromodulation or device-based epilepsy therapies have become a cornerstone of DRE management.
Vagus Nerve Stimulation (VNS) Therapy
For roughly one-third of people living with epilepsy, medication alone doesn’t provide enough control. When seizures continue even after trying two appropriate anti-seizure medications at the right doses, the condition is classified as drug-resistant epilepsy. To address this, the FDA has approved vagus nerve stimulation (VNS) therapy as an alternative treatment.
VNS Therapy, created by LivaNova (NASDAQ: LIVN), is a well-established neuromodulation treatment designed for individuals with drug-resistant epilepsy, especially those with partial or generalized seizures who are not suitable candidates for brain surgery.
In June 2025, LivaNova initiated a formal review with the U.S. Centers for Medicare & Medicaid Services (CMS) to reconsider and potentially broaden Medicare coverage for VNS Therapy. This initiative aims to extend coverage to people with unipolar treatment-resistant depression, signaling the company’s renewed efforts to make this therapy available to more individuals who have not found relief through standard depression treatments.
Back in June 2017, the FDA expanded VNS Therapy’s approval to include children as young as four who have partial-onset seizures that do not respond to medication, making it the first and only device authorized for pediatric drug-resistant epilepsy. Before this expansion, it was limited to patients aged 12 and older.
Dietary Therapies
Doctors often suggest dietary treatments, most notably the Ketogenic diet, to help manage epilepsy, especially in pediatric patients. This high-fat, moderate-protein, very low-carbohydrate diet is typically initiated over a few days. A related but less strict option, the Modified Atkins diet, is also frequently used. Both approaches may help control seizures by lowering blood glucose and insulin while raising ketone levels. Additional lifestyle changes can further reduce exposure to seizure triggers.
Emerging and Pipeline Drug-Resistant Epilepsy Therapies: Toward Disease Modification
The current DRE treatment paradigm is largely palliative and seizure‑centric, focused on suppressing ictal activity rather than modifying the underlying disease process or reversing pharmacoresistance. This is now beginning to change, with a new generation of therapies introducing novel mechanisms and potentially more durable benefits.

Neurona Therapeutics’ NRTX-1001
NRTX-1001 is derived from human stem cells that have been modified to differentiate into interneurons, resembling the brain’s natural inhibitory neurons. These cells produce GABA, a neurotransmitter that helps calm overly active neural circuits and may reduce seizure activity.
In November 2025, Neurona Therapeutics (NMRA) reported that the EMA granted PRIME designation to NRTX-1001 for the treatment of adults with drug-resistant focal epilepsy, underscoring its potential for expedited development and closer regulatory guidance in the EU.
In April 2025, the company reported new findings from its early-phase clinical study of NRTX-1001, an investigational therapy for adults with drug-resistant mesial temporal lobe epilepsy (MTLE). The results were presented at the 2025 American Academy of Neurology Annual Meeting in San Diego, offering encouraging signs of progress for patients with few effective treatment options.
Ramandeep, Senior Consultant of Forecasting and Analytics at DelveInsight, commented that NRTX-1001 represents a paradigm shift in the treatment landscape for drug-resistant focal epilepsy, a patient population historically underserved by both pharmacotherapies and invasive surgical interventions. The cell therapy’s 92% median seizure reduction in the low-dose Cohort 1 during months 7-12, coupled with durable seizure control for 18-24 months post-single-dose administration, positions this therapeutic candidate as a potentially transformative option for patients with mesial temporal lobe epilepsy (MTLE).
He further concluded that the non-destructive mechanism of NRTX-1001 constitutes a distinct competitive advantage over existing surgical options, such as laser ablation and lobectomy, which carry substantial risks of neurocognitive impairment. The preservation of quality-of-life outcomes, evidenced by significantly improved QOLIE scores across all patients in Cohort 1, suggests that NRTX-1001 could address the efficacy-safety dichotomy that has long plagued epilepsy management.
IAMA Therapeutics’ IAMA-6
IAMA-6 is an oral small-molecule therapy developed to selectively block NKCC1 and help normalize neuronal excitability. Overactive NKCC1 has been linked to several disease states, making its inhibition a promising strategy for treating refractory epilepsy and other neurological conditions.
In April 2025, IAMA Therapeutics raised approximately USD 18 million to advance its neuroscience programs, including its lead asset, IAMA-6, which is currently in a Phase I clinical trial (NCT06300398).
Bright Minds Bio’s BM-101
BMB-101 is an innovative, structure-guided agonist of the 5-HT2C receptor that preferentially activates Gq-protein signaling and is developed specifically for chronic neurological conditions in which patients often develop tolerance or reduced responsiveness to therapy. By promoting Gq-pathway activation while minimizing β-arrestin engagement, the drug is intended to limit receptor desensitization and slow the onset of tolerance. This selective signaling approach, applied to a well-established therapeutic target, supports a unique anti-epileptic mechanism designed to provide durable seizure reduction for patients with highly refractory forms of epilepsy.
In January 2026, Bright Minds Biosciences (NASDAQ: DRUG) announced encouraging Phase II BREAKTHROUGH study findings in adults with drug-resistant absence seizures and developmental and epileptic encephalopathies. The data showed median seizure reductions of up to 73%, enhancements in REM sleep, and a favorable safety profile. The company is now preparing for global registrational drug-resistant epilepsy trials.
Looking Ahead: From Seizure Suppression to Precision Care
Across the leading markets, both the diagnosed epilepsy population and the number of patients living with DRE are expected to grow over the coming decade, driven by aging demographics, improved diagnosis and reporting, and longer survival.
Despite these advances, significant unmet needs persist. There is still no therapy approved specifically for “drug‑resistant epilepsy” as a standalone indication; most marketed options are labeled by seizure type or syndrome. Many patients remain only partially controlled, and tolerability, adherence, and access barriers continue to limit real‑world outcomes.
Going forward, the most effective drug-resistant epilepsy treatment strategies are likely to be individualized combinations of optimized pharmacotherapy, timely consideration of surgery or neuromodulation, targeted dietary and lifestyle interventions, and, increasingly, innovative pipeline agents aimed at the core biology of pharmacoresistance.
For clinicians, payers, and industry stakeholders alike, DRE will remain a high‑priority area, both clinically and commercially, as the field moves from incremental seizure reduction toward the longer‑term goal of durable, disease‑modifying control.

Downloads
Article in PDF
Recent Articles
- The Question That Remains Unanswered: What Might Be Causing Alzheimer’s?
- Celiac Disease – Intestinal damage of Gluten
- Which Pharma Companies are Transforming the Drug-Resistant Epilepsy Market Landscape?
- EPIDIOLEX and FINTEPLA in 2026: Commercial Anchors in a Precision DEE Pipeline
- DRUG-RESISTANT EPILEPSY



